Article Text

Abstract
Objective Infection is a major cause of death in patients with SLE. This study aimed to explore the infection rate in patients with SLE receiving a low dose of intravenous cyclophosphamide (IV-CYC).
Methods Clinical parameters of 1022 patients with SLE from 24 hospitals in China were collected. Patients were divided into the short-interval and lower-dose (SILD, 400 mg every 2 weeks) IV-CYC group and the high-dose (HD, 500 mg/m2 of body surface area every month) IV-CYC group. The clinical data and infection rate between the two groups were compared.
Results Compared with HD IV-CYC, the infection rate of the SILD IV-CYC group was significantly lower (13.04% vs 22.27%, p=0.001). Respiratory tract infection (10.28% vs 15.23%, p=0.046) and skin/soft tissue infection (1.78% vs 4.3%, p=0.040) were significantly decreased in the SILD IV-CYC group. Moreover, infections occurred most likely in patients with SLE with leucopenia (OR 2.266, 95% CI 1.322 to 3.887, p=0.003), pulmonary arterial hypertension (OR 2.756, 95% CI 1.249 to 6.080, p=0.012) and >15 mg/day of glucocorticoid (OR 2.220, 95% CI 1.097 to 4.489, p=0.027).
Conclusions SILD IV-CYC showed a lower frequency of infection events than high-dose IV-CYC in patients with SLE.
- SLE
- cyclophosphamide
- therapeutics
Data availability statement
The data used during the current study are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOW ON THIS TOPIC
Infection is the major cause of death in patients with SLE.
Cyclophosphamide is one of the most acknowledged and effective treatments for patients with SLE, while it can increase the susceptibility to infection.
WHAT THIS STUDY ADDS
Short-interval and lower-dose cyclophosphamide (SILD IV-CYC) results in less infection susceptibility compared with high-dose cyclophosphamide.
More infections occurred in patients with SLE with leucopenia, pulmonary arterial hypertension and on glucocorticoids.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
SILD IV-CYC was superior to high dose at less risk of infection.
Introduction
SLE is a serious systemic and chronic autoimmune disease with various clinical features that continue to pose a challenge to developing effective treatments with minimal side effects. It is known that 11%–45% of patients with SLE develop severe infections during treatment.1 In recent decades, numerous studies have presented that infection is one of three major causes of death in patients with SLE.2–4 Some research has also shown that some patients have even experienced more than one severe infection.2 5 Impaired immune functions involving the innate and adaptive immune system are the intrinsic factors of infection vulnerability in patients with SLE.6–8 Moreover, the use of immunosuppressants markedly elevates the risk of infection. To better manage and improve the prognosis of patients with SLE, we conducted a retrospective, real-word, multicentre study on the infection of patients with SLE receiving intravenous cyclophosphamide (IV-CYC) in China.
Materials and methods
Patient population
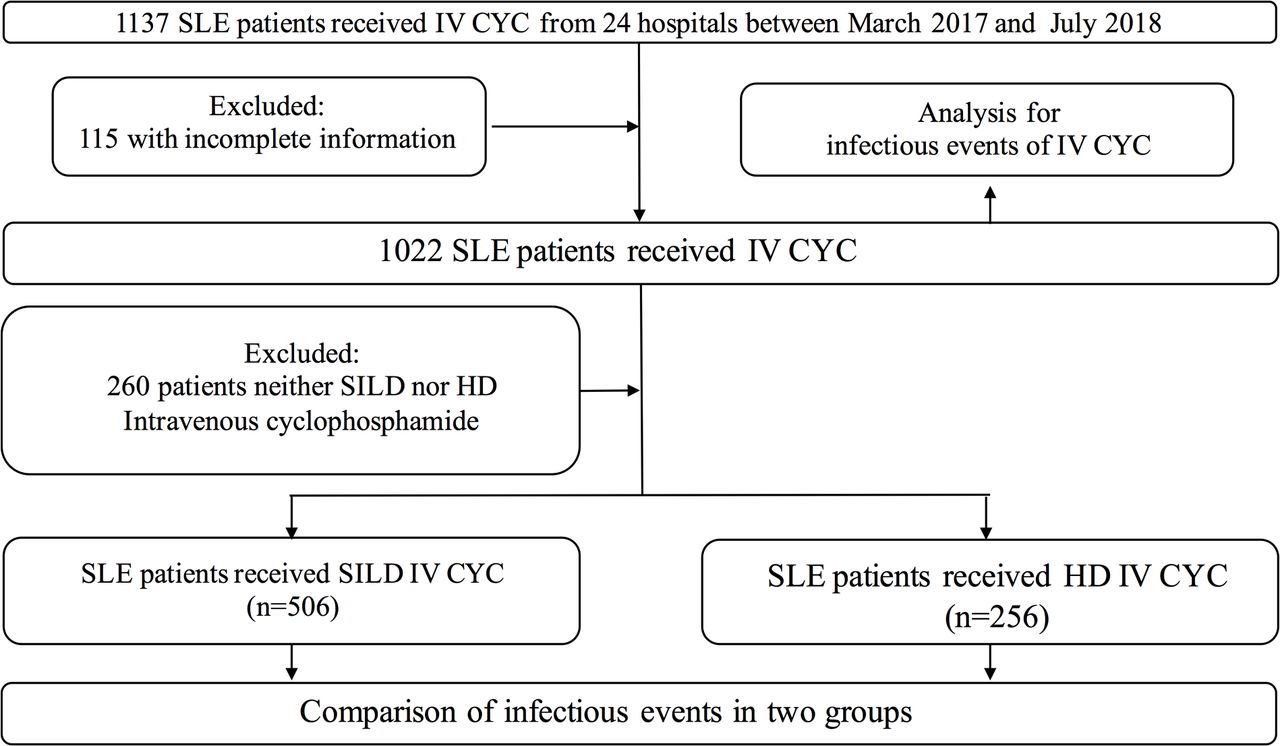
A total of 1137 patients who visited 24 hospitals covering 17 provinces in China from March 2017 to July 2018 were screened (depicted in figure 1) for this study (SILD cohort). All patients with SLE were diagnosed according to the 1997 revised classification criteria of the American College of Rheumatology9 and received IV-CYC. Their medical histories were collected by retrospective survey in the inpatient and outpatient electronic medical records of patients. We excluded 115 patients with incomplete information. Patients in combination with CYC and other immune suppressants (mycophenolate mofetil, azathioprine, ciclosporin, tacrolimus, methotrexate, leflunomide, rituximab, etc) were also excluded from the study. Patients who received glucocorticoid pulse therapy were acceptable. The initial dose of prednisone was 40–60 mg/day in these patients. Finally a total of 1022 patients were included in the study. Of these patients, 506 received short-interval and lower-dose (SILD) IV-CYC treatment every 2 weeks at a fixed dose of 400 mg,10 11 and 256 patients were treated with the high-dose (HD) IV-CYC at a dose of 500 mg/m2 of body surface area every month.12 13

Flow diagram of the selection of patients with SLE. HD IV-CYC, high-dose intravenous cyclophosphamide; IV-CYC, intravenous cyclophosphamide; group 1, the SILD IV-CYC group, short-interval and lower-dose intravenous cyclophosphamide fortnightly with a fixed dose of 400 mg; group 2, the HD IV-CYC group, high-dose intravenous cyclophosphamide monthly at a dose of 500 mg/m2 of body surface area; n, number of patients; SILD IV-CYC, short-interval and lower-dose intravenous cyclophosphamide.
Data collection
The collected demographic data included gender, age of enrolment, age of onset, systemic manifestation (eg, lupus nephritis, neuropsychiatric SLE, interstitial pneumonia, pulmonary arterial hypertension, leucopenia, etc), white cell count, neutrophil count, lymphocyte count, IV-CYC duration, accumulated dose of CYC, glucocorticoid and immunosuppressive agents before intravenous cyclophosphamide, as well as any comorbidities (diabetes mellitus, hypertension, coronary heart disease, hyperlipidaemia, etc) and infection site (respiratory system, digestive system, urinary system, skin, septicaemia, etc). The glucocorticoid pulse therapy, the initial dose of glucocorticoids and the dosage of glucocorticoids at the time of infection were also recorded. The cumulative doses and duration of CYC was from the day of initiation of CYC to the day of infection occurred.
Statistical analysis
Infection events occurring during IV-CYC treatment of the remaining 1022 patients with SLE were recorded, including infection site, duration and cumulative dose of CYC, and risk factors. A comparison of infectious events was made between the SILD IV-CYC group and the HD IV-CYC group.
Patients with an infection that did not require antibiotic treatment were considered to have a mild infection. Those who were treated with antibiotics were regarded as having a moderate infection. Severe infection refers to an infection that leads to hospitalisation, prolonged hospitalisation, life-threatening illness or death.
The Statistical Product and Service Solutions (SPSS) V.26.0 was used to analyse the data. Continuous variables were presented as median (IQR), and statistical significance between two groups was assessed using a Mann-Whitney U test. Categorical data were expressed as absolute count (percentage), and comparison between two groups were made by χ2 or Fisher’s exact test. A stepwise multivariate logistic regression analysis was used to determine the risk factors for infections, and the ORs of the infection event risk and its 95% CIs were calculated. In univariate analysis, the factors related to infection at p<0.15 and diabetes mullitus were entered into the multivariate logistic model. The threshold of significance was set to p<0.05.
Results
The characteristics of patients with SLE are shown in table 1, with the average patient age being 39.00 (30.00–50.00). The duration and cumulative dose of CYC were 6.00 (3.00–10.00) months and 4.80 (2.40–8.00) g, respectively. The most common disease presentations were lupus nephritis (LN) and neuropsychiatric SLE, as well as those impacting the haematologic system and respiratory system. As shown in table 1, there was no significant difference in age, gender, duration of CYC, cumulative dose of CYC, glucocorticoid treatment dose or organ involvement between the patients receiving SILD IV-CYC and HD IV-CYC.
Baseline characteristics of patients with SLE in this study
Infection events in patients with SLE
Infections occurred in 177 (17.32%) of the 1022 patients with SLE included in this study. The most frequently recorded sites of infection were the respiratory tract (12.82%), followed by the skin/soft tissue (2.54%), the urinary tract (1.17%) and the gastrointestinal tract (0.98%). Of these 177 patients, 23 patients experienced more than one infection episode and 17 patients even had two sites of infection during IV-CYC treatment.
The short-interval, lower-dose intravenous cyclophosphamide group showed less infection than the high-dose group
As depicted in table 2, the infection risk was found to be lower in patients who received SILD IV-CYC compared with those treated with HD IV-CYC (13.04% vs 22.27%, p=0.001). The respiratory tract was the most common site of infection in both groups. In the SILD IV-CYC group, the risk of developing either a respiratory tract infection (10.28% vs 15.23%, p=0.046) or skin/soft tissue infection (1.78% vs 4.3%, p=0.040) was significantly decreased. No difference in susceptibility to infection could be detected in the urinary tract, gastrointestinal, central nervous system or bloodstream between the two groups. Although there is no significant difference in the occurrence of mild infection (5.93% vs 9.38%) and severe infection (2.37% vs 4.30%) between the two groups, the moderate infection rate was lower in the SILD IV-CYC group (4.74% vs 8.59%, p=0.035).
Sites and severity of infection for patients with SLE in each group
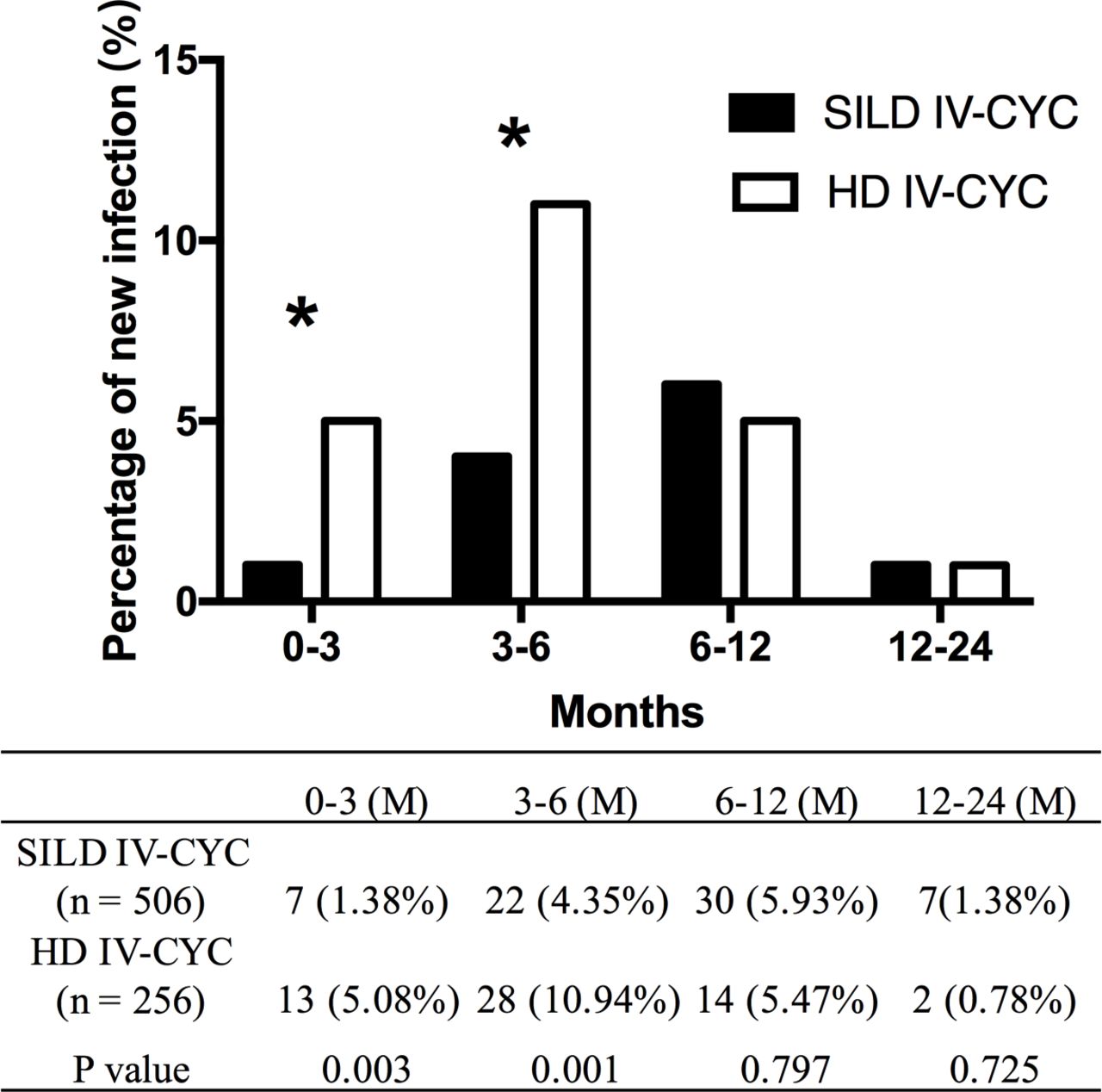
Most of the infections occurred within 6 months (104/177, 58.76%) and 1 year (167/177, 94.35%) of IV-CYC injection. After 6 months of IV-CYC injection, the infection rates in the SILD group and the HD group were 5.73% (29/506) and 16.02% (41/256) (p=0.000), respectively, and after 12 months of IV-CYC injection, the infection rates in the SILD group and HD group were 11.66% (59/506) and 21.48% (55/256), respectively. During the treatment period of 0 to 6 months, the infection events in the HD IV-CYC group increased significantly compared with the SILD IV-CYC group (figure 2).
{kind=link}
{kind=link}
Comparison of the rates of new infection in patients with SLE undergoing SILD IV-CYC and HD IV-CYC treatments. HD IV-CYC, high-dose intravenous cyclophosphamide; M, months; SILD IV-CYC, short-interval lower-dose intravenous cyclophosphamide.
In addition, when a multivariate analysis was performed (table 3), the risk of infection in patients with SLE who received HD IV-CYC was found to be twice than that of those who had received SILD IV-CYC (OR 2.018, 95% CI 1.315 to 3.097, p=0.001).
Risk factors for infection in patients with SLE receiving IV-CYC
Other risk factors of infection
As shown in table 3, patients with SLE who also had leucopaenia (OR 2.266, 95% CI 1.322 to 3.887, p=0.003) or pulmonary arterial hypertension (OR 2.756, 95% CI 1.249 to 6.080, p=0.012) were more susceptible to infection. There was no significant difference in glucocorticoid usage between patients with SLE who developed infections and those who did not. However, all of the patients with SLE were divided into three groups according to the dosage of glucocorticoids they received: those free of glucocorticoids, glucocorticoids ≤15 mg/day and glucocorticoids >15 mg/day. The multivariate logistic regression analysis found that when the dose of glucocorticoid was >15 mg/day, the risk of infection was higher (OR 2.220, 95% CI 1.097 to 4.489, p=0.027). Other factors that were valuable in univariate analysis, including CYC accumulation, CYC duration and lymphocytopaenia, did not confer any additional infection risk.
Discussion
Infection is one of the most critical causes of death in patients with SLE. This study is a real-world, multicentre study that has shown the infection risk associated with IV-CYC. Consistent with various studies,14 15 leucopaenia, lymphopaenia and neutropaenia are associated with an increased risk for infection in patients with SLE. Our results confirm that patients with SLE who also have leucopenia are more vulnerable to infection after receiving IV-CYC.
Along with the impaired immune functions associated with SLE, the use of immunosuppressive drugs containing CYC additionally increases the susceptibility to infection in patients with SLE.16 17 CYC is one of the most acknowledged and successful therapies for treating SLE, especially for severe, organ-threatening SLE, and has been shown to dramatically improve the prognosis of these patients. Since the 1970s, a series of clinical trials carried out by the National Institutes of Health have shown that the intermittent infusions of CYC with prednisone was superior to a single application of prednisone.12 13 18 When CYC was first used to treat SLE, HD IV-CYC was the standard therapy for LN in the induction phase. In recent years, many studies have demonstrated that SILD IV-CYC is also efficacious, and there was no difference between the SILD IV-CYC and HD IV-CYC groups in SLE disease control.10 11 19 20 However, the side effects of long-term exposure to CYC have been shown to include infection, bone marrow damage, malignancy, ovarian dysfunction and haemorrhagic cystitis at any therapeutic dose. The infection occurring in associated with CYC treatment could be fatal for patients with SLE. Our previous randomised, single-centre study showed that patients with SLE receiving SILD CYC treatment had fewer infection events compared with the HD CYC group; however, the differences did not reach statistical significance.10 In the Euro-Lupus Nephritis Trial study, episodes of severe infection were more than twice as frequent in the HD CYC group.11 In the present study, we have shown that the risk of infection was significantly lower in patients with SLE in the SILD IV-CYC group than in the HD IV-CYC group. The infection risk of HD IV-CYC is 2.018 times higher than that of SILD IV-CYC after adjusting by the duration and accumulated dose of CYC, pulmonary arterial hypertension, leucopaenia and lymphocytopaenia.
In addition, we observed that patients who received IV-CYC with glucocorticoids >15 mg/day had a higher infection risk. Our data also showed that most infections occurred within the first 6 months of IV-CYC treatment. This may be due to most patients with SLE also being on glucocorticoids >15 mg/day in addition to IV-CYC during the first 6 months of the induction phase. Fortunately, patients who received SILD IV-CYC remained at low infection risk throughout our study.
Our study has inherent limitations of retrospective research. First of all, it was not recorded for research purposes, and some clinical details such as infectious organisms are incomplete. Second, the regimens of glucocorticoids were inconsistent in the study, and some patients also received intravenous pulse methylprednisolone therapy at the beginning of the treatment. Glucocorticoids at the time of infection were analysed; however, the cumulative and average dose of glucocorticoids and other factors which may affect the risk of infection could not be obtained. Last, patients who lost follow-up were excluded, and there might be some selection bias among the study subjects.
In summary, we found that the infection rate of patients with SLE treated with SILD IV-CYC is much lower than that of patients treated with HD IV-CYC. This indicates that SILD IV-CYC could be a better option in the treatment of patients with SLE.
Data availability statement
The data used during the current study are available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. The approval (reference no 2015PHB004-01) was obtained from the Peking University People’s Hospital Ethics Committee for this study. Participants gave informed consent to participate in the study before taking part.
References
Footnotes
Contributors ZL and RL (guarantor) conceived the study and revised the manuscript. MS analysed, interpreted the patient data and was a major contributor in writing the manuscript. MM and XZ recorded the patient data. The rest of the authors contributed to patient data collection. All authors approved the submitted version.
Funding The work was supported by the National Natural Science Foundation of China (grant no 32000639 and 82171772) and Peking University People’s Hospital Research and Development Funds (grant no RS2020-01).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.