Article Text

Statistics from Altmetric.com
SLE is a disease of immune dysregulation and complex interactions of genetics, hormones and environmental factors lead to loss of self-tolerance with aberrant immune responses of the innate and adaptive immune systems. It is well documented that viral infections including coronaviruses are an environmental factor that contributes to the development of autoimmunity. However, data regarding the impact of COVID-19 pandemic in patients with SLE are scarce. It is not known if COVID-19 triggers SLE. We read with great interest the study by Favalli et al, in which the authors considered that the real incidence of COVID-19 in patients with SLE remains to be clarified at present.1 The impact of COVID-19 in their patients with SLE was very low. Their preliminary data do not seem to suggest an increased risk of SARS-CoV-2 infection for patients with SLE.
The causality of the association between SLE and COVID-19 has not been established. The observational associations may be biased by confounding and reverse causality. Mendelian randomisation (MR) analysis is widely used to assess the presence of causal relationships between genetic variants and selected outcome, independent of factors that may interfere with observational studies. Here, we leverage data from large-scale genetic association studies to verify the authors’ findings and identify genetic proxies for SLE and apply in MR analyses to investigate their causality with COVID-19.
Summary statistics of SLE were obtained from the IEU OpenGWAS project,2 which included 5201 SLE cases versus 9066 population controls. Summary-level genetic data for COVID-19 were acquired from The COVID-19 Host Genetics Initiative genome-wide association meta-analysis.3 Three COVID-19 traits were selected: COVID-19 (RELEASE 5), which included 38 984 COVID-19 cases versus 1 683 768 population controls; COVID-19 (hospitalised vs population) RELEASE 5, which included 9986 hospitalised COVID-19 cases versus 1 877 672 population controls; COVID-19 (very severe respiratory confirmed vs population) RELEASE 5, which included 5101 very severe respiratory confirmed COVID-19 cases versus 1 388 342 population controls. The IEU GWAS ID were respectively ebi-a-GCST011073, ebi-a-GCST011081 and ebi-a-GCST011075. The MR analyses were performed using the inverse-variance weighted method. All summary data used in this study are publicly available and were obtained with the consent and ethical approval of the relevant participants.
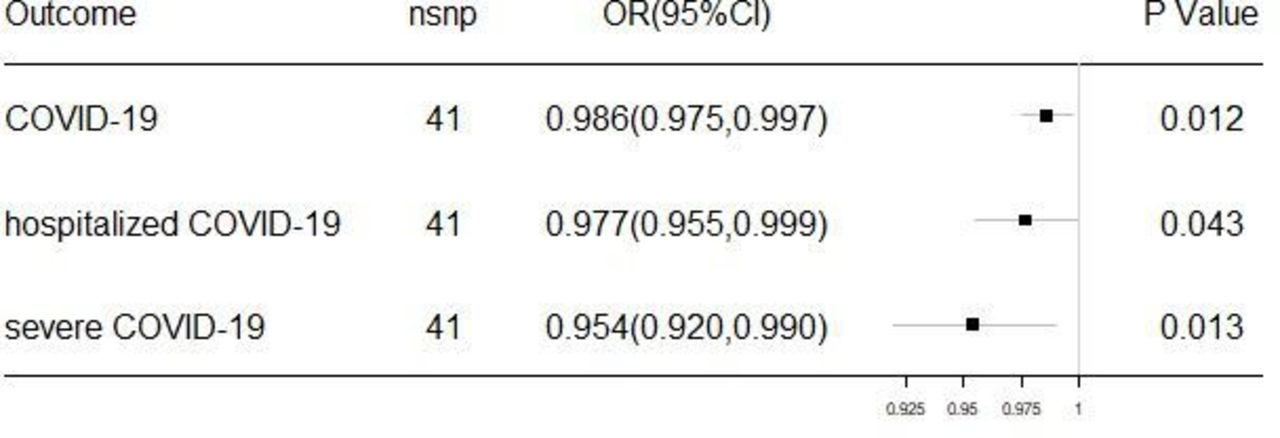
The MR analyses (figure 1) showed that there were consistent evidences that SLE are causally associated with COVID-19 (OR 0.986, CI 0.975 to 0.997, p=0.012), hospitalised COVID-19 (OR 0.977, CI 0.955 to 0.999, p=0.043) and severe COVID-19 (OR 0.954, CI 0.920 to 0.990, p=0.013). Our results showed the potential association between SLE and COVID-19 and revealed that genetic predisposition to SLE could lower the risk of COVID-19, hospitalised COVID-19 or severe COVID-19. The reverse MR study was also performed. It shows that genetic predisposition to COVID-19 was not causally associated with the risk of SLE, COVID-19 (OR 0.911, CI 0.423 to 1.963, p=0.811), hospitalised COVID-19 (OR 1.208, CI 0.881 to 1.657, p=0.241) and severe COVID-19 (OR 0.886, CI 0.676 to 1.160, p=0.378).

{kind=link}
Mendelian randomisation analysis of SLE and outcome. SNP, single-nucleotide polymorphism.
The immune response is an important determinant in viral infections including coronaviruses. Most patients with SLE have evidence of high type I interferon activity, which may theoretically act as an antiviral line of defence.4 Anti-rheumatic drugs, such as hydroxychloroquine and baricitinib, have been identified as possible targets for COVID-19 treatment due to their proposed antiviral effects.5 Hydroxychloroquine has shown several antiviral mechanisms, including the inhibition of inflammatory cytokines such as IL-1, IL-6 and TNF-alpha.6
MR has limitations including genetic confounding, and issues related to heterogeneity across different tissues and populations. Further investigations should be encouraged to be carried out with a larger sample size which can give robust casual estimates.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Footnotes
SR and LP contributed equally.
Contributors These authors contributed equally: SR and LP.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.