Article Text

Abstract
Objective Lupus nephritis is one of the most common and serious complications of systemic lupus erythematosus (SLE). Lupus nephritis is a major cause of kidney failure in patients with SLE, attributed to increased morbidity and mortality. The in situ deposition of intrarenal immune complexes promotes the accumulation of inflammatory cells and causes kidney injury.
Methods We here extracted transcriptome array datasets for expression of complement molecules in human lupus nephritis. Furthermore, we performed gene set enrichment analysis to identify molecular signatures associated with follow-up kidney function in lupus nephritis.
Results Within the glomerular compartment, intrarenal mRNA expression levels of C3AR1 (p=0.0333) and C5AR1 (p=0.0167) correlated with treatment success reflected by kidney function recovery specifically in class III lupus nephritis, while no such association was observed in class II or class IV lupus nephritis. Interestingly, mRNA expression levels of either glomerular C3AR1 or C5AR1 resulted in identical gene set and signalling pathways enrichments in human lupus nephritis, including interferon signalling and signalling by interleukins. Direct comparison of C3AR1 and C5AR1 confirmed a strong association between glomerular mRNA expression levels of both complement receptors (r=0.8955, p<0.0001).
Conclusions This study provides additional insights into signalling pathways associated with intrarenal synthesis of complement components in lupus nephritis that might be also affected by targeted therapy of the complement system. These results require confirmation but may contribute to a personalised treatment approach in distinct classes of human lupus nephritis.
- Lupus Nephritis
- Lupus Erythematosus, Systemic
- Autoimmune Diseases
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Not applicable.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Lupus nephritis is one of the most common and serious complications of systemic lupus erythematosus, attributed to increased morbidity and mortality.
The in situ deposition of intrarenal immune complexes promotes the accumulation of inflammatory cells and causes kidney injury in lupus nephritis.
WHAT THIS STUDY ADDS
We here show that intrarenal expression of complement receptor C3AR1 and C5AR1 is correlated with treatment success specifically in class III lupus nephritis.
Intrarenal expression of both complement receptors were strongly correlated among one another with identical molecular signatures in human lupus nephritis that involve interferon signalling and signalling by interleukins.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The fact that intrarenal synthesis of C3AR1 and C5AR1 correlated with treatment success specifically in class III lupus nephritis may indicate that a more personalised treatment approach may be rational.
Furthermore, the overlapping molecular signatures between glomerular C3AR1 and C5AR1 expression could imply that blocking both complement receptors may have additional effects.
Introduction
Lupus nephritis is one of the most common and serious complications of systemic lupus erythematosus (SLE).1 Lupus nephritis is a major cause of kidney failure in patients with SLE, attributed to increased morbidity and mortality.2 Lupus nephritis classification has last been updated in 2018.3 Class I lupus nephritis (minimal mesangial) has a prevalence of 1% in adults and represents <20% of all cases of nephrotic syndrome that undergo renal biopsy.4 5 Class II lupus nephritis (mesangial proliferative) accounts for 7%–22% of all cases and generally presents with isolated haematuria, low-grade proteinuria and normal renal function.6–8 It is considered mild, but it is associated with the risk of further progression to focal or diffuse class III/IV lupus nephritis.9 10 Classes III and IV lupus nephritis (focal and diffuse proliferative glomerulonephritis) is most prevalent and associated with the highest risk of progressive kidney disease requiring prompt immunosuppressive treatment.8 Class V lupus nephritis (membranous glomerulopathy) is presenting with nephrotic range or non-nephrotic proteinuria and often associated with proliferative forms.11 12 Class VI lupus nephritis (advanced sclerosing) is defined by more than 90% of sclerotic glomeruli, often resulting in impaired renal function and variable amount of proteinuria.
The in situ deposition of intrarenal immune complexes promotes the accumulation of inflammatory cells and causes kidney injury especially in active classes III and IV lupus nephritis.13 14 Among them, complement system activation with decreased serum levels of complement C3 and C4 have been found in about 75% of patients with SLE with focal nephritis and 90% in patients with diffuse nephritis.15 In addition, colocalisation of immunoglobulin isotypes IgG, IgA and IgM along with C1q, C3 and C4 in the glomerular compartment is almost exclusively present in patients with lupus nephritis.16 Among potential sources of intrarenal complement deposits, the concept of intrarenal complement synthesis has been described more than three decades ago in experimental lupus nephritis.17 Because protein-based detection methods of intrarenal deposits cannot dissect between these sources of complement components, we have previously analysed transcriptome datasets to systematically describe glomerular synthesis of complement components in lupus nephritis.18 However, relevance of glomerular complement synthesis with regard to treatment response and progression of lupus nephritis remains elusive. Therefore, we here aimed to expand our current knowledge about intrarenal complement synthesis associated with treatment success reflected by recovery of kidney function in human lupus nephritis.
Methods
Data extraction from Nephroseq
Transcriptome array datasets were used from Nephroseq (www.nephroseq.org, June 2022, University of Michigan, Ann Arbor, Michigan, USA). Particularly, median-centred log2 mRNA expression levels (GSE32591, platform: Affymetrix Human Genome U133 Plus 2.0 Array, altCDF v10) were extracted specifically from microdissected glomerular and tubulointerstitial compartments from lupus nephritis samples with available data for lupus nephritis class and glomerular filtration rate (GFR) slope (class II: n=6, class III: n=6, class IV: n=12, online supplemental figure 1 and tables 1–3).19 According to Nephroseq, delta GFR slope corresponds to the last GFR value according to modification of diet in renal disease obtained from the patient minus the first GFR value (at time of biopsy), divided by the number of years of follow-up.
Supplemental material
Gene set enrichment analysis
For gene set enrichment analysis, the whole dataset (14 samples from healthy living donors, 32 samples with lupus nephritis) were included, and genes co-expressed with glomerular mRNA expression of C3AR1 (reporter: 209906_at) and C5AR1 (reporter: 220088_at) were extracted from Nephroseq (www.nephroseq.org, June 2022, University of Michigan, Ann Arbor, Michigan, USA, online supplemental table 4). Co-expression analysis for tubulointerstitial C9 (reporter: 206727_at) was not available from Nephroseq (www.nephroseq.org, November 2022, University of Michigan, Ann Arbor, Michigan, USA). Candidate genes with a correlation threshold of ≥0.5 were used for pathway analysis with reactome (http://reactome.org) with a predefined entities value of p≤0.0010.20
Statistical methods
Variables were tested for normal distribution using the Shapiro-Wilk test. Statistical comparisons were not formally powered or prespecified. Categorical variables are presented as frequency and percentage, mean±SD are shown for normally distributed values, and median (IQR) for non-normally distributed values. Spearman’s correlation was performed to assess the correlation between GFR slopes and median-centred log2 mRNA expression levels, and the direct comparison between glomerular mRNA expression levels of C3AR1 (209906_at) and C5AR1 (220088_at). Heatmaps reflecting the mean values of Spearman’s ρ are shown, the asterisks indicating statistical significance correlations. For group comparisons, the Mann-Whitney U test was used to determine differences in medians. Data analyses were performed with GraphPad Prism (V.9.3.1 for macOS, GraphPad Software, San Diego, California, USA). Stepwise multiple regression analyses were performed using IBM SPSS Statistics (V.27 for MacOS, IBM Corporation, Armonk, New York, USA). We retained covariates significantly associated with GFR slope in a multivariable regression model, limiting the model covariates to avoid model overfit. A probability (p) value of <0.05 was considered statistically significant.
Results
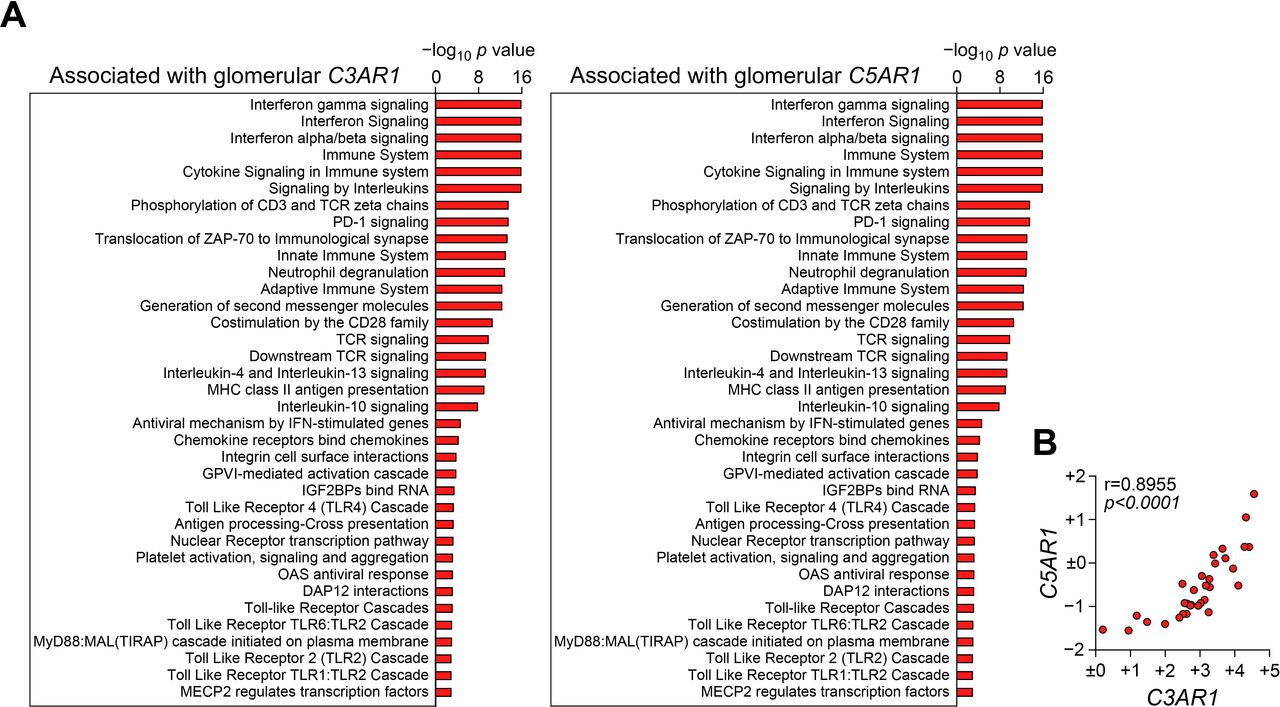
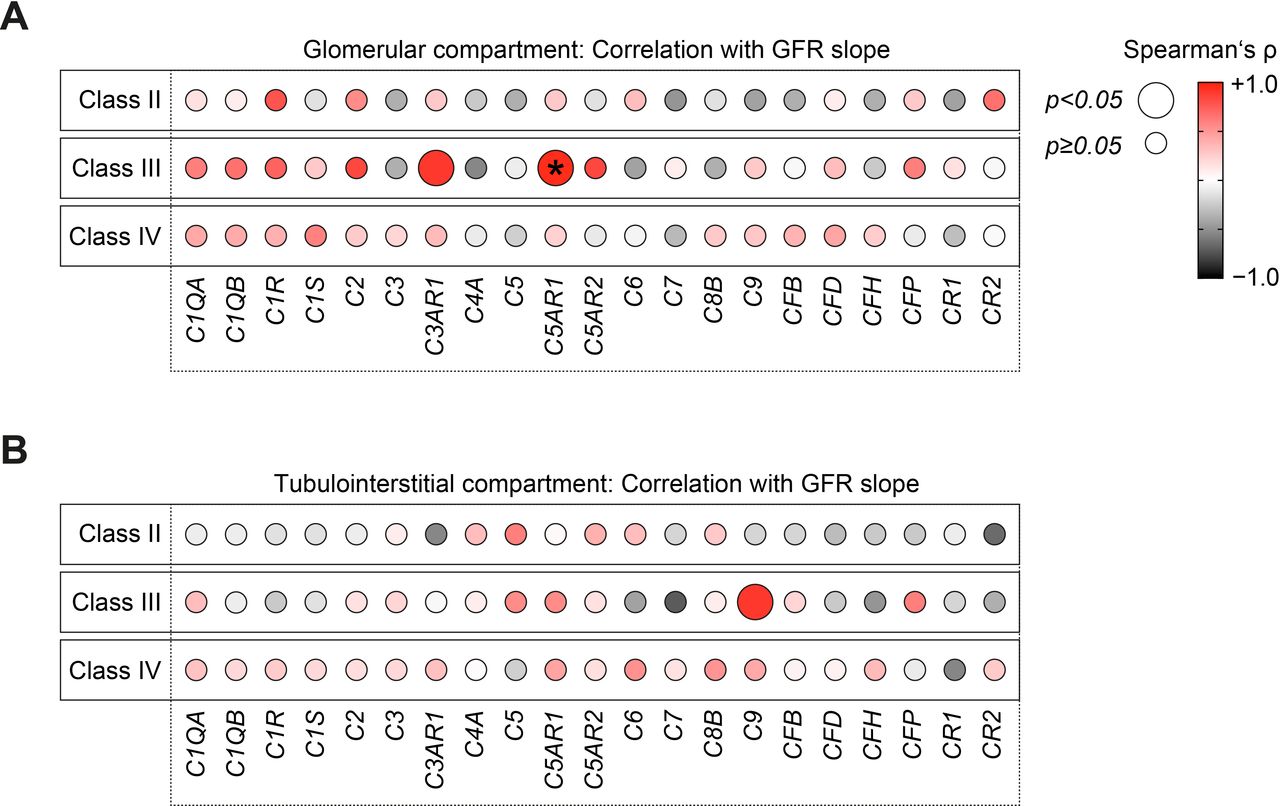
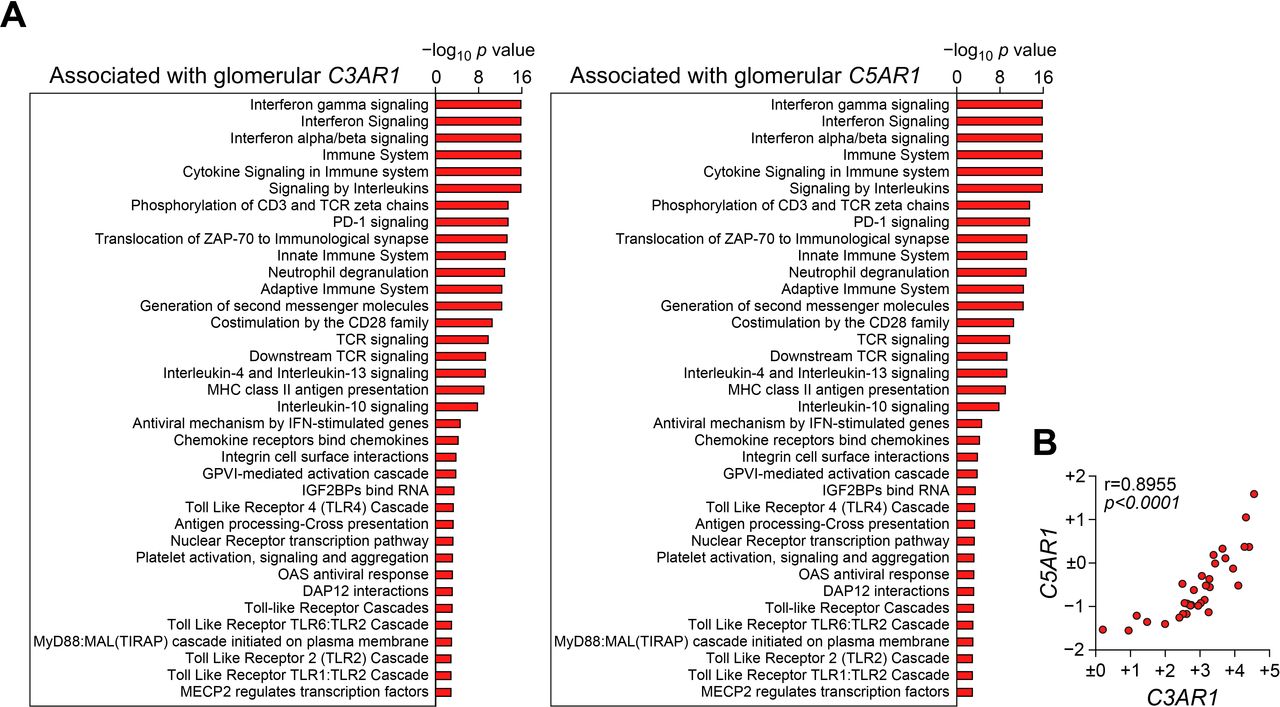
We first compared intrarenal mRNA expression levels of complement components in class II, class III and class IV lupus nephritis with GFR slope per year. Within the glomerular compartment, intrarenal mRNA expression levels of complement receptors C3AR1 (p=0.0333) and C5AR1 (p=0.0167) correlated with a positive correlation with GFR slope per year specifically in class III lupus nephritis (figure 1A). Interestingly, no such association was observed in class II or class IV lupus nephritis (figure 1A). Within the tubulointerstitial compartment, specifically mRNA expression levels of complement C9 correlated with positive GFR slope specifically in class III lupus nephritis (figure 1B). Multiple regression analysis confirmed that glomerular C5AR1 was the main denominator of positive eGFR slope in class III lupus nephritis (glomerular C3AR1: β=0.2934, p=0.7906, glomerular C5AR1: β=0.923, p=0.0087; tubulointerstitial C9: β=0.0737, p=0.8855, figure 1A,B). Because glomerular C3AR1 had no independent association with GFR slope, we next aimed to identify molecular signatures associated with these complement receptors in lupus nephritis. Interestingly, mRNA expression levels of either glomerular C3AR1 or C5AR1 resulted in identical gene set and signalling pathways enrichments (figure 2A). Glomerular expression of both complement receptors correlated with enrichment of interferon signalling and signalling by interleukins in lupus nephritis (figure 2A). Direct comparison of C3AR1 and C5AR1 confirmed a strong association between glomerular mRNA expression levels of both complement receptors (r=0.8955, p<0.0001, figure 2B). In summary, we here describe that glomerular expression of complement receptor C5AR1 associated with positive GFR slope specifically in class III lupus nephritis. Furthermore, intrarenal expression of complement receptors C3AR1 and C5AR1 were strongly correlated among one another with identical molecular signatures in human lupus nephritis.

Intrarenal expression of complement molecules associated with progression of lupus nephritis. (A, B) Correlations between GFR slope and mRNA expression levels of distinct complement molecules are shown separated for the glomerular and tubulointerstitial compartment in human lupus nephritis (class II: n=6, class III: n=6, class IV: n=12) are shown by heatmaps reflecting mean values of Spearman’s ρ. Circle size represents significance level in the univariate analysis, asterisk (*) in the multivariate analysis. GFR, glomerular filtration rate
{kind=link}
{kind=link}
Molecular signatures associated with glomerular expression of complement receptors C3AR1 and C5AR1 in human lupus nephritis. (A) Entities -log10 p values of signalling pathways separated for gene set enrichment associated with either glomerular C3AR1 or C5AR1 mRNA expression are shown. (B) Spearman’s correlation was performed to directly compare median-centred log2 mRNA expression levels of glomerular C3AR1 and C5AR1 expression. DAP12, DNAX-activating protein of 12 kDa; GPVI, glycoprotein VI; IFN, interferon; IGF2BP, Insulin-like growth factor 2 mRNA-binding protein; MAL, MyD88 adaptor-like; MECP2, methyl CpG binding protein 2; MHC, major histocompatibility complex; MYD88, myeloid differentiation primary response 88; OAS, oligoadenylate synthetase; PD-1, programmed cell death protein-1; TCR, T-cell receptor; TIRAP, TIR domain-containing adaptor protein; ZAP-70, zeta-chain-associated protein kinase-70.
Discussion
In experimental and human lupus nephritis, the complement system has a protective role mediated by cell death and circulating immune complex clearance.21 22 In addition, complement system activation and the in situ deposition of immune complexes from the circulatory system or kidney may promote the accumulation of inflammatory cells and cause kidney damage in lupus nephritis.14 While the role of the complement system in the pathogenesis of lupus nephritis has long been described, its paradoxical effects on disease activity make it a challenging therapeutic target. Therefore, a detailed knowledge about the role of distinct complement components is essential for complement targeted therapy in lupus nephritis.
We have previously identified accelerated intrarenal synthesis of distinct classical and alternative complement pathway components to associate with impaired kidney function.18 We here expand our current knowledge, providing evidence that intrarenal expression of distinct complement pathway components is also correlated with progression of lupus nephritis. Particularly, glomerular expression of complement receptors C3AR1 and C5AR1 associated with positive GFR slope specifically in class III lupus nephritis. Blocking C3 and C5 complement receptors have been shown to protect from experimental lupus nephritis.23 24 Combined with our observations that both complement receptors showed a positive correlation with GFR slope, this may implicate a link between glomerular expression of complement receptors C3AR1 and C5AR1 and treatment success in lupus nephritis. Upregulation of C3 and C5 complement receptors has already been described in experimental lupus nephritis and observed in the initial phase of kidney injury, supporting an involved in disease development.23 24 This experimental data is in line with our observation that glomerular C3AR1 and C5AR1 expression correlated with treatment success specifically in focal class III lupus nephritis (representing early proliferative glomerulonephritis affecting fewer than 50% of the glomeruli) and not in diffuse class IV lupus nephritis (representing later stage proliferative glomerulonephritis affecting 50% or more of the glomeruli). Classes III and IV lupus nephritis are distinguished quantitatively because it is considered that there is a continuum for severe lupus nephritis with segmental lesions.25 However, not all cases of class III lupus nephritis progress towards class IV.26 Indeed, classes III and IV lupus nephritis have various subtypes, such as endocapillary glomerulonephritis, necrotising crescentic glomerulonephritis associated with anti-neutrophil cytoplasmic antibody, renal vascular lesions including thrombotic microangiopathy and focal segmental glomerulosclerosis associated with lupus podocytopathy.27–30 Moreover, we here identified that intrarenal expression of both complement receptors were strongly correlated among one another with identical molecular signatures in human lupus nephritis that involve interferon signalling and signalling by interleukins. This is in line with observations in animal models reporting that interferon gamma signalling was required for development of experimental lupus nephritis.31 Because blocking C3 and C5 complement receptors have been shown to protect from experimental lupus nephritis, these complement receptors are an attractive therapeutical target in human lupus nephritis.23 24 The fact that intrarenal synthesis of C3AR1 and C5AR1 correlated with treatment success specifically in class III lupus nephritis may indicate that targeting the complement system may vary between distinct classes of human lupus nephritis, and a more personalised treatment approach may be rational. Furthermore, the overlapping molecular signatures between glomerular C3AR1 and C5AR1 expression could imply that blocking both complement receptors may have additional effects. This is of particular interest since ongoing trials are currently testing efficacy and safety of anti-C5 antibody (NCT04564339) and C5a receptor (C5aR) antagonists (NCT02151409) in patients with lupus nephritis.
In summary, this study provides additional insights into signalling pathways associated with intrarenal synthesis of complement components in lupus nephritis that might be also affected by targeted therapy of the complement system. Because this study included only a limited patient number with no detailed analysis regarding individual treatment regimens or additional outcome parameters (particularly proteinuria), these results require confirmation but may contribute to a personalised treatment approach in distinct classes of human lupus nephritis.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Not applicable.
Ethics statements
Patient consent for publication
Ethics approval
Data was extracted from Nephroseq Research Edition (Ann Arbor, Michigan: University of Michigan; available from: www.nephroseq.org).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors BT conceived the study, analysed data and wrote the manuscript. DT performed gene set enrichment analysis. SH edited the manuscript. All authors reviewed and approved the manuscript’s content before submission. BT is the author acting as guarantor.
Funding We acknowledge support by the Open Access Publication Funds of the Göttingen University.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.