Article Text

Abstract
Purpose Voclosporin is a novel calcineurin inhibitor approved in the United States in January 2021 for the treatment of adult patients with active lupus nephritis in combination with background immunosuppressive therapy. The Phase 3 AURORA 1 study showed that adding voclosporin to mycophenolate mofetil (MMF) and low-dose steroids led to significantly greater reductions in proteinuria at 52 weeks. Given the potentially serious safety concerns associated with the long-term use of oral steroids, we evaluated the safety and efficacy of treatment with voclosporin in patients maintained on low-dose steroids for an additional 24 months in the AURORA 2 continuation study.
Methods Key inclusion criteria for the parent AURORA 1 study included biopsy-proven active lupus nephritis (Class III, IV, or V ± III/IV), proteinuria ≥1.5 mg/mg (≥2 mg/mg for Class V) and estimated glomerular filtration rate (eGFR) >45 mL/min/1.73 m2. Patients who completed AURORA 1 were eligible to enroll in AURORA 2 on the same blinded treatment of voclosporin or placebo in combination with MMF (target dose 2 g/day) and low-dose oral steroids. Per-protocol steroid use in AURORA 1 required a rapid taper from a starting dose of 20–25 mg/day to a target of ≤2.5 mg/day by Week 16. The final dose of steroids in AURORA 1 was the initial starting dose in AURORA 2; the dose could then be adjusted further at the discretion of the study investigator. AURORA 2 was not designed nor powered to address the impact of voclosporin on oral steroid dose.
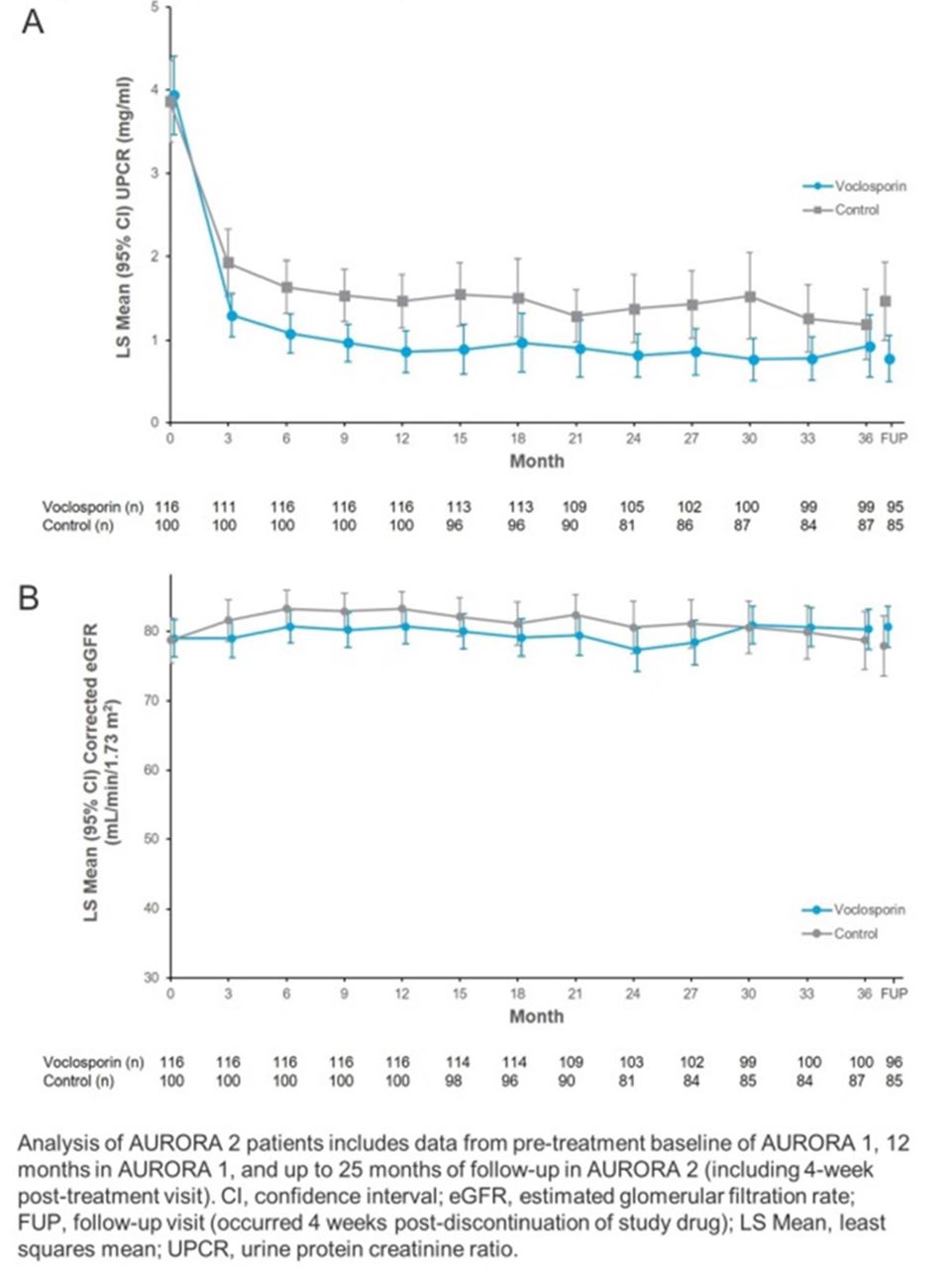
Results In total, 116 patients in the voclosporin arm and 100 patients in the control arm enrolled in AURORA 2. The efficacy observed in patients treated with voclosporin in AURORA 1 was maintained throughout AURORA 2 as indicated by the greater Least Square (LS) mean reductions in UPCR from baseline in the voclosporin arm vs. control arm at all time points (Figure 1A). The overall exposure to oral steroids during the study was similar for both treatment arms; over three years of treatment, the majority of patients were on steroid doses ≤2.5 mg/day (Table 1). There were no new or unexpected safety signals detected in patients who continued on voclosporin treatment compared to control-treated patients with similar rates of serious adverse events in the voclosporin (18.1%) and control arms (23.0%). There were no deaths in the voclosporin arm during AURORA 2; four deaths were reported in the control arm (pulmonary embolism [n=1], coronavirus infection [n=3]). Mean eGFR remained stable throughout the study (Figure 1B).
{kind=link}
A) UPCR and B) eGFR over time
Oral steroid use
Conclusions Voclosporin was safe and well-tolerated over three years of treatment with a similar safety profile to control and no unexpected safety signals detected. Further, the significant reductions in proteinuria initially achieved in AURORA 1 were maintained in AURORA 2 even in the absence of traditional high-dose steroids. These data provide evidence of a long-term treatment benefit of voclosporin in patients with lupus nephritis and also support the use of lower doses of steroids in the treatment of this disease.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.