Article Text

Abstract
Background Systemic lupus erythematosus (SLE) is an autoimmune disease which generally affects young woman. Kidney affection appears in around 40% of patients and eventually condition the prognosis. Mortality is bimodal: initially is secondary to infections and disease activity and, subsequently, is caused by cardiovascular events (CVE).
In recent years, responsible causes of this increase of cardiovascular risk (CVR) in SLE have been evaluated. In turn, chronic kidney disease is an independent cardiovascular risk factor and is a possible outcome in lupus nephritis.
Objective To describe the prevalence of CVE in a cohort of SLE patients and to establish differences according to whether renal involvement is present.
Methods Descriptive, cross-sectional, interventional study including SLE patients according to SLICC/ACR 2012 criteria. Two distinct groups were included: SLE with non-renal affection (group 1) and SLE with renal affection (group 2). Classic CV risk factors, established CVD, concomitant diseases, disease activity, current therapy and previous therapeutic history were collected. Established CVD is defined by myocardial infarction (AMI), stroke and/or peripheral arteriopathy (PA).
Carotid ultrasound (US) was performed to each patient to measure intima-media thickness (IMT) at different levels: common carotid, carotid bulb and internal carotid; according to current US values for measuring IMT: normal <0.9 mm; increased >0.9 mm and IMT >1.3 is indicative of atheroma.
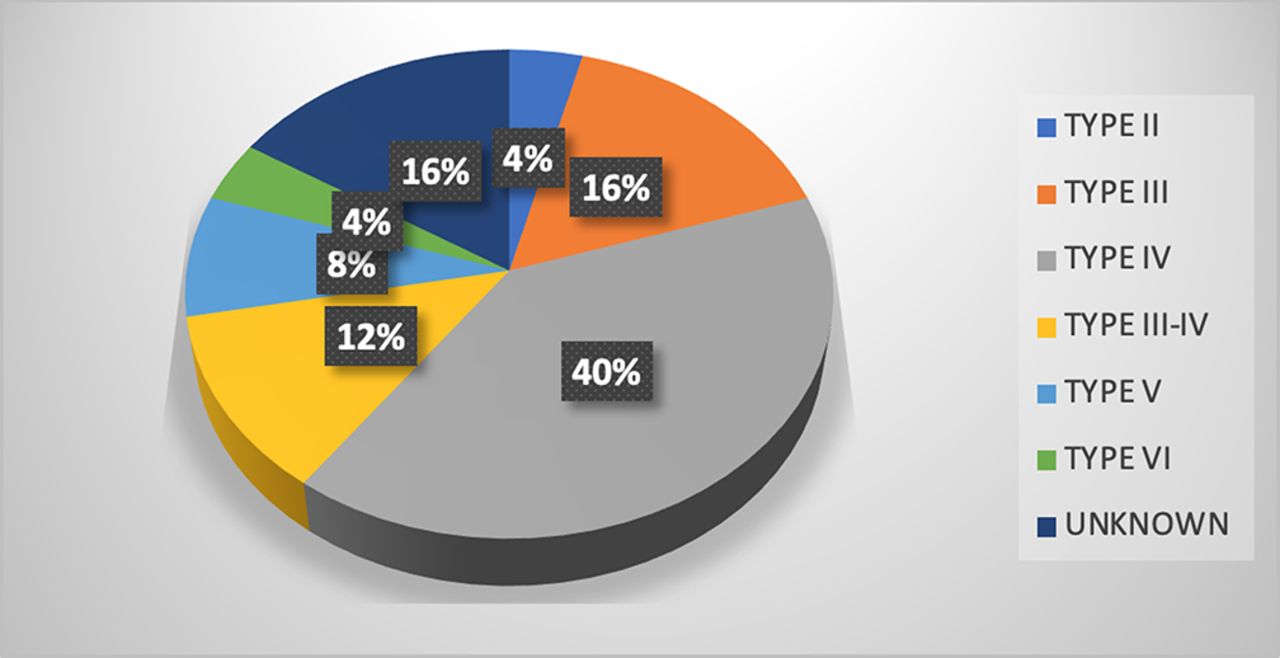
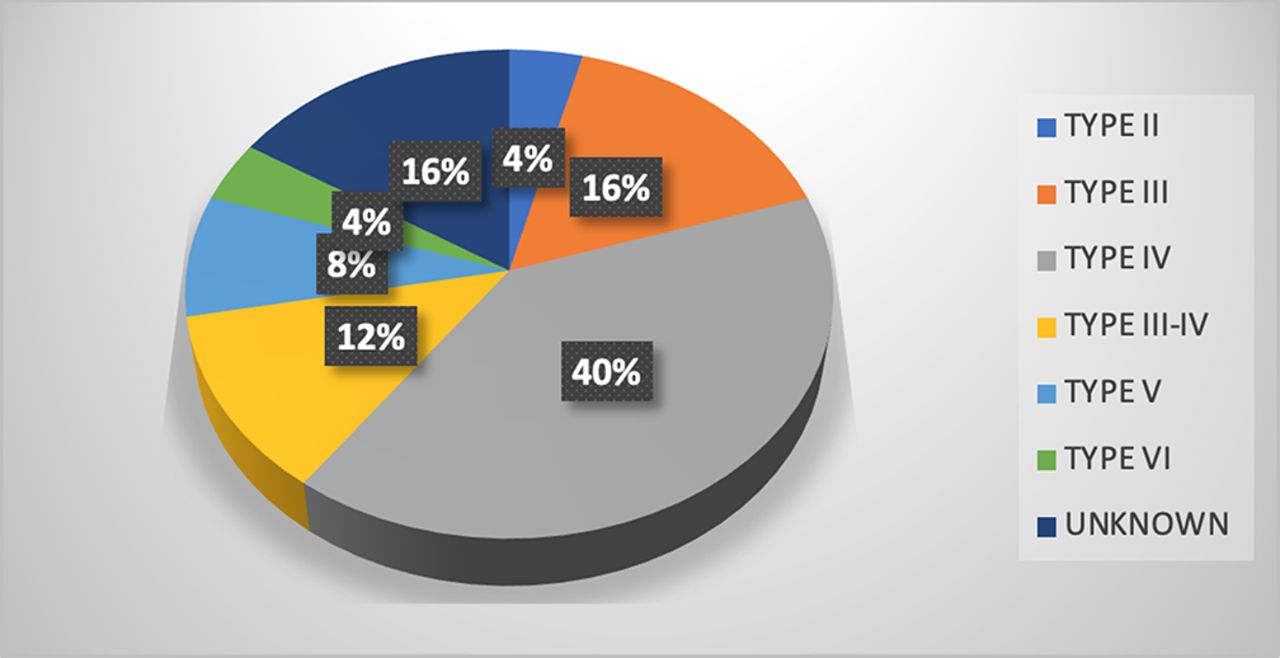
Results 133 patients (91.04% women) with a median age of 51.19 (14.52) years and 17.21 (11.02) years since diagnosis were included. 32 of them (24.06%) had renal involvement as glomerulonephritis (GN) evidenced by biopsy (18.66%), urine sediment and/or 24-hour urine sample alterations (2.99%) or end-stage renal failure (2.24%). Prevalence of different types of GN is shown in the figure.
Figure1 Prevalence of different types of GN.
In group 1, patients with high blood pressure, dyslipidemia and diabetes were 30.69%; 39.60% and 6.93%, respectively. Numerically, in group 2 proportion of distinct RCVF was higher: high blood pressure 68.75%, dyslipidemia 46.88% and diabetes 15.63%.
Over the course of the disease, 24.75% of patients in group 1 presented some CVE: AMI (3.96%), stroke (4.95%) and PA (15.84%) whereas this proportions in group 2 were: AMI (6.25%), stroke (6.25%) and PA (9.38%). Out of the total sample, 16.42% patients had an altered carotid doppler US, 4 of them with kidney involvement. In group 1, 14.85% had an increased IMT and 15.84% presented PA, 4.95% developed stroke and 3.96% AMI. In group 2, only 4 patients had anomalies in doppler ultrasound, 3 of them presented PA, 2 developed stroke and 2 AMI. Finally, 21.05% did not undergo carotid US for different reasons.
{kind=link}
Conclusions In our study, no significant statistical differences were found between both groups 1 and 2 referring to development of CVE: AMI (p 0.58), stroke (p 0.77) and PA (p 0.36).
Regarding to the result of doppler US, we observed no differences in terms of increased IMT and development of CVE in both groups: AMI (p 0.38), stroke (p 0.38) and PA (p 0.66).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.