Article Text

Abstract
Purpose Lupus nephritis (LN) is a major clinical challenge and cause of significant morbidity and mortality in systemic lupus erythematosus (SLE). Today >180 SLE risk loci at Genome-wide significance (GWS, p < 5×10–8), including risk genes involved in B-cell function, have been identified. Associations between an individual’s genetical burden and clinical manifestations in SLE can be studied using a polygenic risk score (PRS). In this study, we investigated associations between two SLE B-cell PRSs, SLE ACR-82 classification criteria, dsDNA antibodies and LN.
Methods Female SLE patients (n=1256) and healthy controls (n=519) from Scandinavia were genotyped using Illumina’s Global Screening Array. Two PRSs were calculated1 for each individual, one including 21 GWS risk loci for SLE in genes assigned to B-cell related pathways (SLE B-cell PRS) according to the Kyoto encyclopedia of genes and genomes, Gene Ontology and Reactome databases, and one including a subset of 12 of these loci, limited to B-cell activation pathways (SLE B-cell activation PRS). High and low PRSs were defined as PRSs in the highest quartile and in quartile 1–3, respectively, and groups were compared by logistic regression (SPSS, version 28.0.1.0). A p-value < 0.05 was considered significant.
Results In total, 30% of patients had nephritis according to the ACR-82 criteria with an average age at nephritis onset of 33 years and dsDNA antibodies were more prevalent among patients with nephritis (78%) compared with patients without nephritis (56%) (OR 2.8 (2.0–3.9), p=2.1×10–10). The mean SLE B-cell PRS was higher in cases 2.9 (2.9–3.0) than controls 2.7 (2.6–2.7), (p = 4.1×10–11) and 11% of patients had an SLE B-cell PRS above the 95th percentile of controls. SLE was more prevalent in individuals with a high compared with a low SLE B-cell PRS (OR 1.8 (1.4–2.4), p=4.0×10–6).
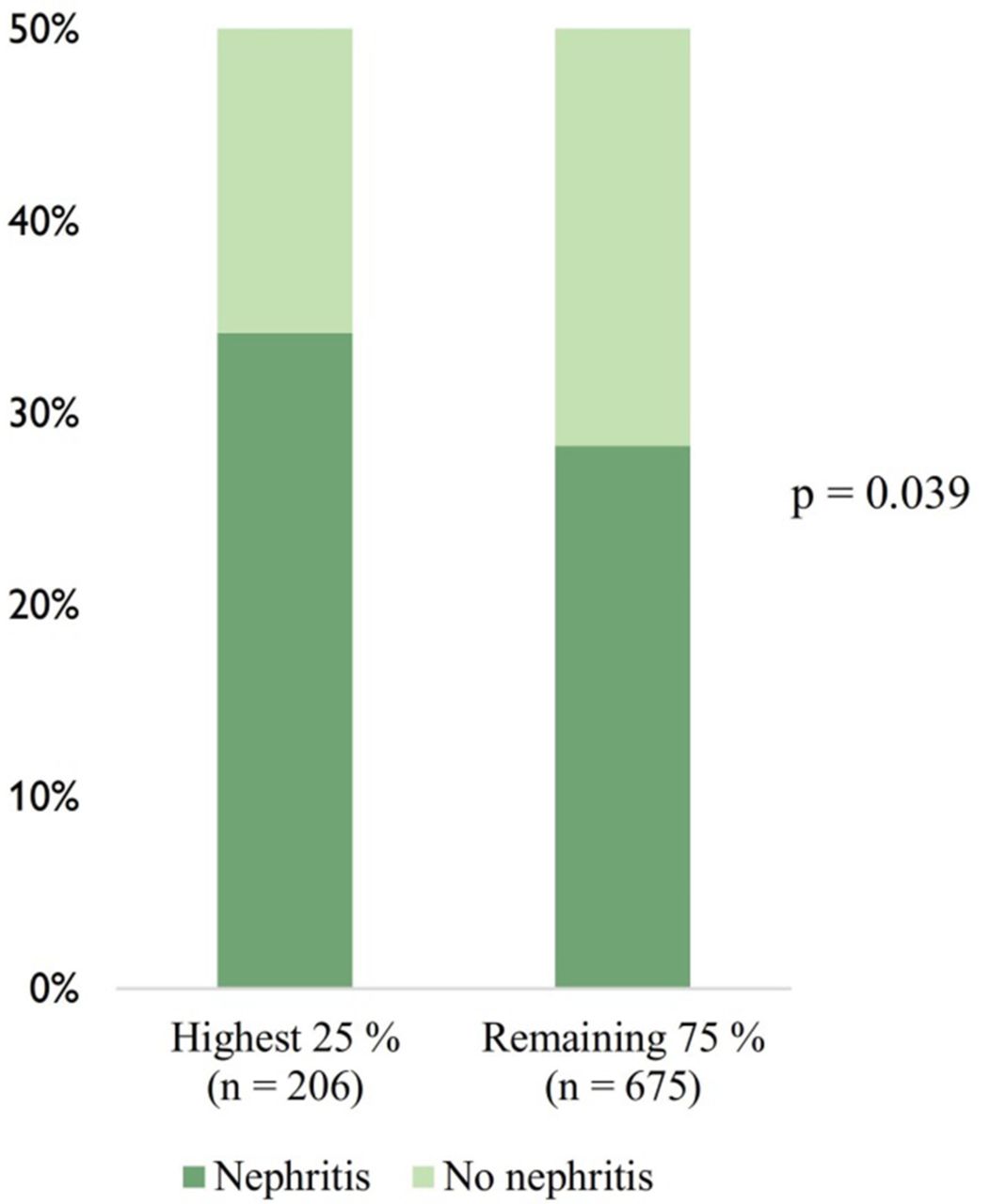
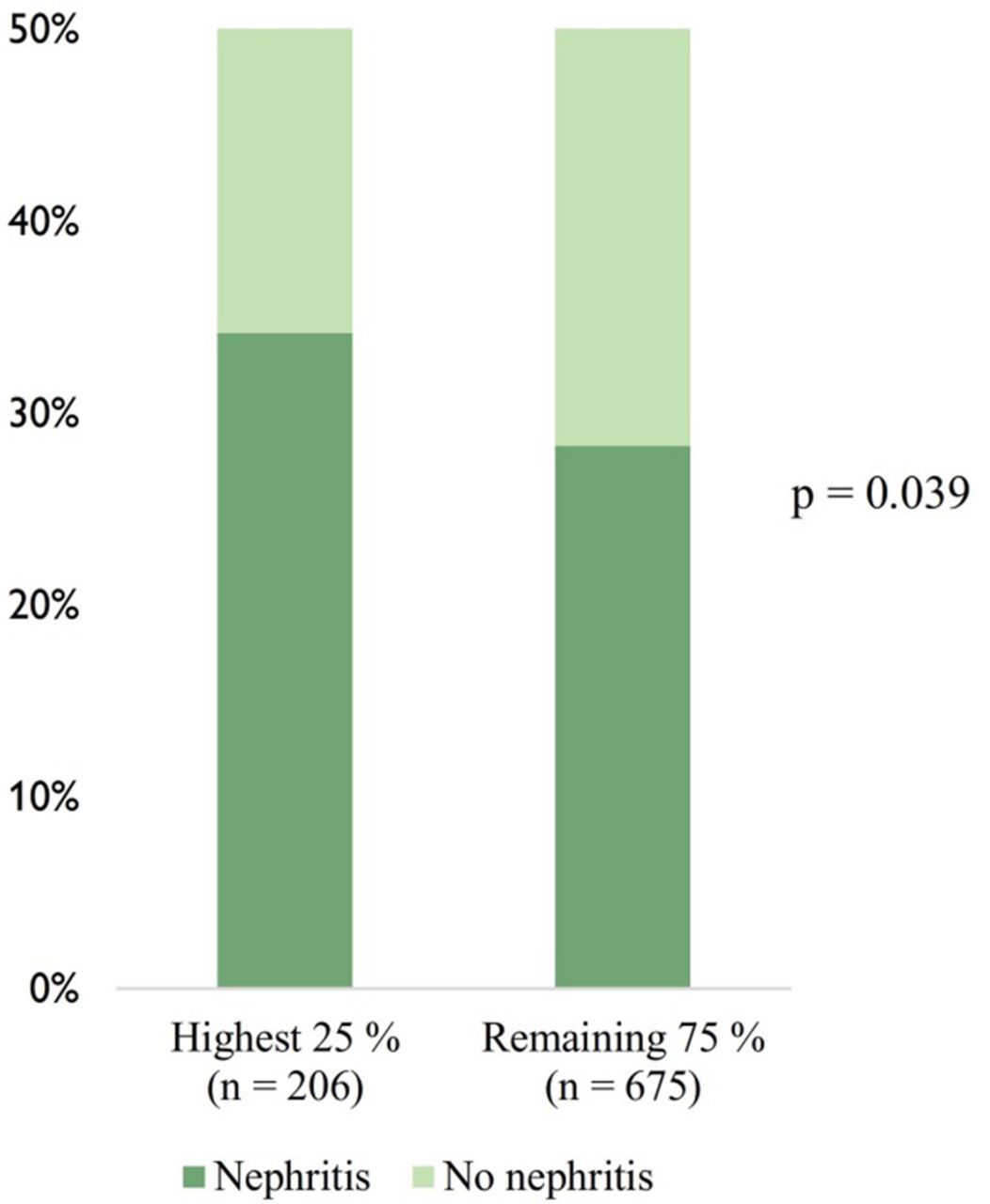
The immunological criterion (ACR-82) was more prevalent among patients with a high compared with low SLE B-cell PRS (OR 1.4 (1.1–1.9), p = 0.013) and a similar association was found for dsDNA antibodies (OR 1.5 (1.1–2.0), p = 0.017). Numerically, a higher prevalence of nephritis was observed in patients with high compared with low SLE B-cell PRS, but it did not reach statistical significance (OR 1.2 (0.9–1.6), p = 0.19). However, the prevalence of nephritis was higher in patients with a high compared with a low SLE B-cell activation PRS (OR 1.3 (1.0–1.8), p = 0.039), Figure 1.
{kind=link}
Prevalence of nephritis in patients with a B-cell activation PRS above the third quartile compared with patients in lower quartiles
Conclusions High SLE polygenic risk related to B cell function is associated with development of dsDNA antibodies and nephritis in SLE. Assessing B-cell PRSs can be important in order to determine the immunologic pathways influencing the disease and to predict clinical phenotype.
References
Reid, S. et al. High genetic risk score is associated with early disease onset, damage accrual and decreased survival in systemic lupus erythematosus. Ann Rheum Dis 2020;79, 363–369.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.