Article Text

Abstract
Objectives In daily practice, the squeeze test is used to screen for arthritis in metacarpophalangeal (MCP) and metatarsophalangeal (MTP) joints. This cross-sectional cohort study determined the diagnostic accuracy of this test.
Methods Patients referred with arthralgia of recent onset that had either a clinical suspicion for progression to arthritis or clinically apparent arthritis were studied. The main outcome was swelling at physical examination of ≥1 MCP or MTP joint. Joint inflammation detected at extremity MRI was the secondary outcome.
Results Both at MCP and MTP joints, a positive squeeze test associated with swollen joints (p<0.005). The sensitivity of the test at the MCP joints was 53%, specificity 82%, positive likelihood ratio (LR+) 3.0, negative likelihood ratio (LR−) 0.6 and area under the receiver operator characteristic curve (AUC) 0.68. At the MTP joints, the sensitivity was 54%, specificity 74%, LR+ 2.1, LR− 0.6 and AUC 0.64. With MRI-detected inflammation as outcome, the sensitivity and specificity were 39% and 86% and 31% and 69% for the test at the MCP and MTP joints, respectively.
Conclusions A positive squeeze test is associated with local joint inflammation but the sensitivity is low, indicating a high percentage of swollen joints with a negative squeeze test. When the test is used on its own, it is insufficient to detect early arthritis.
- Rheumatoid Arthritis
- Early Rheumatoid Arthritis
- Magnetic Resonance Imaging
Statistics from Altmetric.com
Introduction
Convincing evidence has shown that a short symptom duration at the start of the treatment associates with better outcomes of rheumatoid arthritis (RA).1–5 The need to start antirheumatic treatment early calls for the need to identify RA early.6 Adequate collaboration between general practitioners (GPs) and rheumatologists is required to prevent delay in the diagnostic process. Accurate interpretation of palpation of joints (the gold standard to identify arthritis) requires expertise, especially when synovitis in small joints is subtle, which is the case in imminent and early RA. Expertise by rheumatologists is obtained during years of training. For GPs, another method is required to screen for arthritis. Ideally such a test is easy to perform, takes little time and is cheap and accurate.
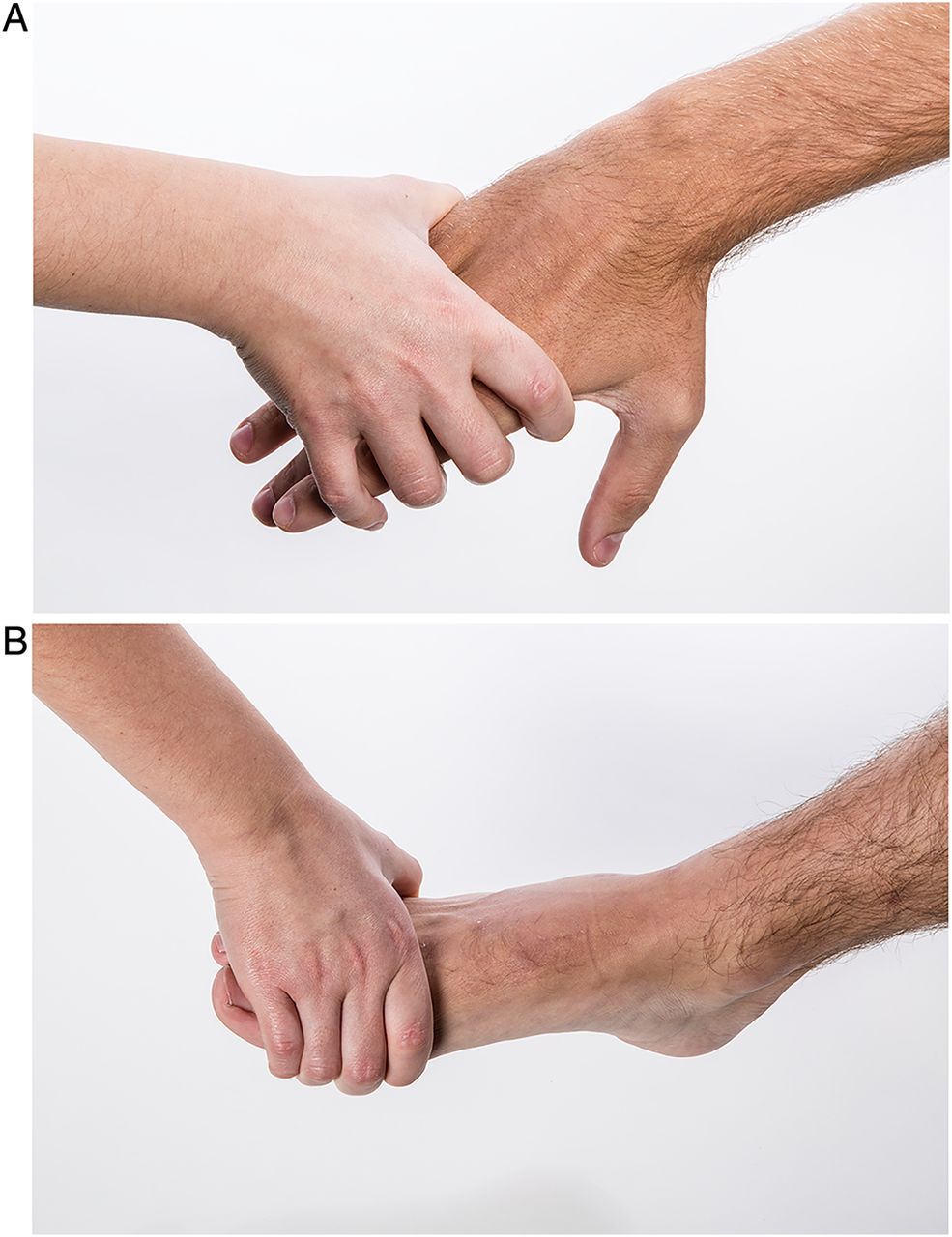
Presently no generally accepted test for early identification of arthritis (other than joint palpation) exists. However, the use of the squeeze test to identify arthritis in metacarpophalangeal (MCP) and metatarsophalangeal (MTP) joints is well promoted by experts and societies such as Arthritis Research UK and the National Rheumatoid Arthritis Society (NRAS).7–12 The test involves squeezing the hand or foot across the knuckle joints (figure 1); if this is unduly painful, it raises the suspicion of arthritis in at least one of the joints that are compressed. This test is simple to perform, rapidly done and cheap, illustrating its utility. There is surprisingly little data on the diagnostic accuracy. Although one study observed, within patients with classified RA, a moderate correlation between a positive squeeze test and tenderness at local palpation of joints,13 the accuracy of the squeeze test to identify arthritis in MCP or MTP joints has never been studied. Therefore, this study aimed to determine the accuracy of the squeeze test to identify early arthritis.

The squeeze test at the metacarpophalangeal joints of the hand (A) and the metatarsophalangeal joints of the foot (B).
Methods
Setting
This cross-sectional study was performed at a rheumatology outpatient clinic with a low referral threshold for GPs (Leiden University Medical Center). To get patients with suspicion on arthritis or RA as soon as possible at the outpatient clinic, close collaboration with local GPs and an Early Arthritis Recognition Clinic14 are present.
Subjects
Included were patients referred with arthralgia of recent-onset (symptom duration <2 years) and either arthritis confirmed at physical examination (arthritis was allowed to be present in any joint and not confined to hand or foot joints) or a clinical suspicion to progress to arthritis over time according to their rheumatologists.15 Patients with arthralgia that at first visit had diagnoses that were clearly other than suspected arthritis or apparent arthritis were not studied as there was no medical need to perform the squeeze test. The patients studied were included between August–October 2013 and November 2013–March 2014; collected data of the patients included from the end of October until mid November were lost due to a technical problem in the MRI scanner.
To determine the reference value for abnormal MRI inflammation (the secondary outcome), MRIs were made of healthy volunteers. Forty-seven symptom-free volunteers were recruited from October 2013 to March 2014 by advertisements in local newspapers. They were age-matched, had no history of joint diseases, no joint symptoms during the last month and no abnormalities at joint examination that was done prior to the MRI.
Assessments and outcomes
The primary outcome was arthritis of MCP or MTP joints at physical joint examination by rheumatological experts; this is the gold standard to identify arthritis. To capture subclinical joint inflammation, MRI-detected inflammation rheumatoid arthritis MRI score (RAMRIS) was studied as secondary outcome. Contrast-enhanced MRI is more sensitive in detecting joint inflammation in wrist and MCP joints than physical examination.16 ,17 Importantly, however, the diagnostic value of MRI is not yet established and the value of MRI of the foot particularly is relatively unexplored. Symptom-free volunteers were scanned to define ‘abnormal MRI inflammation’. Per patient one hand and foot were studied. The squeeze test, joint examination and MRI reading were done by different experts, without knowledge of each other's findings, ensuring maximal blindness (for more detailed description on the assessment of the test and on MRI examination, see online supplementary methods).
Analyses
The MRI inflammation score18 ,19 at MCP(2–5) was the sum of MRI synovitis scores, bone marrow oedema (BME) scores and tenosynovitis scores. For MTP(1–5), synovitis and BME scores were summed; tenosynovitis was not scored as no validated method for the foot exists. Mean scores of both readers were analysed. Continuous data were compared using Mann–Whitney U tests. Then continuous data were dichotomised. If ≥1 MCP joint or ≥1 MTP joint was swollen, this group of joints was categorised as ‘positive’. The cut-off for a positive MRI was defined as the score that was present in <5% of age-matched symptom-free volunteers; this stringent criterion was chosen to prevent false positive scan results. This was a score of 5.0 and 3.0 for the MCP joints and MTP joints, respectively. IBM SPSS statistics V.20 was used.
Results
In the indicated periods, 152 patients were eligible and studied; online supplementary table S1 presents their characteristics. In total, 25% of patients had a positive squeeze test at MCP joints, 31% a positive squeeze test at MTP joints and 14% a positive squeeze test at MCP and MTP joints. Within the patients with symptoms of their hand (MCPs/proximal interphalangeal joints (PIPs)), the squeeze test was positive in 36.8%; within the patients with symptomatic forefeet, the squeeze test was positive in 48.9%.
Accuracy of the squeeze test with joint swelling at physical examination as outcome
Patients with a positive MCP squeeze test had more swollen MCP joints than patients with a negative test 0.97 (SD 1.42) vs 0.21 (SD 0.66) (p<0.001, figure 2A). Similarly, patients with a positive MTP squeeze test had more swollen MTP joints (0.83 (SD 1.46) vs 0.24 (SD 0.74), p=0.004).

{kind=link}
{kind=link}
Number of metacarpophalangeal (MCP) (A) and metatarsophalangeal (MTP) joints (B) that were inflamed at physical examination and the MRI inflammation scores in MCP (C) and MTP joints (D) in patients with a negative and positive squeeze test. The dotted line indicates the cut-off that was chosen to dichotomise the data. For swelling of MCP and MTP joints, this cut-off was ≥1. For MRI inflammation on the MCP joints, the cut-off for a positive MRI was ≥5 and for the MTP joints it was ≥3. The mean number of swollen MCP joints in the MCP squeeze test negative group (n=114) was 0.21 (SD 0.66) and that in the MCP squeeze test positive group (n=38) was 0.97 (SD 1.42, p<0.001). The mean number of swollen MTP joints in the MTP squeeze test negative group (n=105) was 0.24 (SD 0.74) and the mean in the test positive group (n=47) was 0.83 (SD 1.46, p=0.004). In case of a positive MCP squeeze test (n=38), the mean MRI inflammation score was 6.8 (SD 4.2); and in case of a negative squeeze test (n=114), this was 4.4 (SD 3.7, p<0.001). In case of a positive MTP squeeze test, the mean MRI inflammation score was 3.4 (SD 3.1) and for the negative squeeze test group 3.2 (SD 3.2, p=0.61).
Subsequently, the data on swollen joints were dichotomised. Patients with a positive MCP squeeze test had more often arthritis in ≥1 MCP joint than patients with a negative test (OR 5.2, 95% CI 2.2 to 12.2). A similar observation was done for the MTP joints (OR 3.3, 95% CI 1.4 to 7.8, table 1A). The sensitivity of the squeeze test at the MCP joints was 53% , specificity 82%; positive likelihood ratio (LR+) 3.0 and negative likelihood ratio (LR−) 0.6. For the MTP joints, the sensitivity was 54%, specificity 74%, LR+ 2.1 and LR− 0.6. The area under the receiver operator characteristic curve (AUC) of the squeeze test for arthritis of MCP joints was 0.68 (95% CI 0.56 to 0.79) and of MTP joints 0.64 (95% CI 0.52 to 0.76).
Test characteristics and discriminative ability of the squeeze test performed at all metacarpophalangeal (MCP) and metatarsophalangeal (MTP) joints studied (A,B) or in symptomatic hands and forefeet only (C,D) with the presence of joint swelling at physical examination (A,C) or the presence of MRI-detected inflammation (B,D) as outcomes
Association between squeeze test and inflammation on MRI
The secondary outcome was MRI-detected local inflammation. A positive MCP squeeze test was associated with a higher MRI inflammation score than a negative test (p<0.001, figure 2C); this is in contrast to the MTP squeeze test. A positive squeeze test at the MCP joints was associated with an odds of 3.9 (95% CI 1.8 to 8.4) on local inflammation at MRI. The MCP squeeze test had a sensitivity of 39%, specificity 86%, LR+ 2.8 and LR− 0.7 (table 1B). The specificity, sensitivity, LR+ and LR− of the MTP squeeze test were 69%, 31%, 1.0 and 1.0, respectively.
Subanalyses
Of each patient, one hand and one foot were studied. Consequently, not all hands and feet that were evaluated were symptomatic. To determine whether the diagnostic accuracy was different when only symptomatic hands/feet were assessed, all analyses were repeated in patients with hand symptoms (MCP or PIP) or forefoot symptoms; this showed similar results (table 1C, D).
Analyses were also stratified for ACPA and sex; results for the MCP test were comparable, but the accuracy was less for the MTP test in ACPA-positive and male patients (see online supplementary table S2).
Finally, analyses on the MCP squeeze test were repeated with the individual MRI inflammation features as outcomes to explore whether the test was associated with MRI-depicted synovitis, tenosynovitis or BME. The results remained almost similar, although the accuracy was slightly less when MRI-detected BME was used as outcome (see online supplementary table S3).
Discussion
The present study determined the diagnostic accuracy of the squeeze test for identification of arthritis and showed that the sensitivity is rather low and the specificity moderate. The diagnostic accuracy of the squeeze test at the hands was slightly higher than that at the forefeet.
GPs need tools to select patients with an increased chance on early arthritis. The squeeze test is widely advocated to this end (eg, in the S-factor campaign of the NRAS12). A screenings test requires a high sensitivity to prevent false negatives. In this study, up to 50% of the patients with swollen MCP or MTP joints at physical examination were missed by the squeeze test. This finding may be in contrast with what is commonly assumed. Alternatively, it might also not be expected that a rather simple test, evaluating pain in a group of joints, correlates perfectly with swelling of individual joints.
Although physical examination performed by trained rheumatologists is the golden standard to identify arthritis, in case of subtle abnormalities clinicians may differ in their sensitivity in recording arthritis. MRI-detected joint inflammation was studied as secondary outcome. MRI is more sensitive in detecting joint inflammation.16 ,17 However, the specificity of MRI-detected inflammation is not yet known. To prevent false positive MRI findings, MRIs of age-matched asymptomatic volunteers were used to define a MRI reference.
A positive MTP squeeze test was associated with arthritis of MTP joints at physical examination but not with MRI-detected inflammation. The cause of this discrepancy is unclear. Absence of evaluation of MRI-detected tenosynovitis at MTP joints is likely not the single explanation. Notably a recent study showed a poor correlation of MRI-detected inflammation with joint swelling at physical examination at MTP joints (but not at MCP joints),16 and the diagnostic value of forefoot MRI is still undetermined. For unknown reasons, the accuracy of the MTP squeeze test was also less in ACPA-positive and male patients. Altogether the MTP squeeze test seemed less reliable than the MCP squeeze test.
We did not study the squeeze test in GP practices. Then the prevalence of observed arthritis at physical examination will be considerably lower, and the sensitivity and specificity vary with prevalence.20 The positive and negative likelihood ratios are more robust against differences in prevalence of outcomes. Nonetheless, a LR+ of 2 or 3 and a LR− of 0.6 indicate only a small increase and decrease in the probability on arthritis.
In conclusion, clinical evaluation is the basis of medicine. From many simple tests, the test characteristics are insufficiently known. The present study showed that the squeeze test correlated moderately with joint examination. Up to 50% of swollen MCP or MTP joints was missed by the squeeze test. Therefore, the squeeze test should be combined with other tests to achieve a good discriminative ability. Unfortunately, a combination of tests that are cheap, easy to perform and also accurate in discrimination still needs to be developed. At present, clinicians should keep in mind the test characteristics of the squeeze test when performing this test in daily practice.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online tables
Footnotes
Handling editor Tore K Kvien
Contributors WBvdB and LM shared first authorship based on equal contribution. WBvdB, LM and AHMvdH-vM designed the study. WBvdB and LM collected data and performed analyses. MR and TWJH provided advice during the study. AHMvdH-vM supervised the study. WBvsB drafted the manuscript. All authors contributed to the manuscript and approved the final manuscript.
Funding Vidi grant of the Netherlands Organisation for Scientific Research.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Medical ethical committee of the LUMC.
Provenance and peer review Not commissioned; externally peer reviewed.