Article Text

Abstract
Objective: To examine if, in systemic lupus erythaematosus (SLE), exposure to immunosuppressive therapy (cyclophosphamide, azathioprine, methotrexate) increases cancer risk.
Methods: A case–cohort study was performed within a multi-site international SLE cohort; subjects were linked to regional tumour registries to determine cancer cases occurring after entry into the cohort. We calculated the hazard ratio (HR) for cancer after exposure to an immunosuppressive drug, in models that controlled for other medications (anti-malarial drugs, systemic glucocorticoids, non-steroidal anti-inflammatory drugs (NSAIDs), aspirin), smoking, age, sex, race/ethnicity, geographic location, calendar year, SLE duration, and lupus damage scores. In the primary analyses, exposures were treated categorically (ever/never) and as time-dependent.
Results: Results are presented from 246 cancer cases and 538 controls without cancer. The adjusted HR for overall cancer risk after any immunosuppressive drug was 0.82 (95% CI 0.50–1.36). Age ⩾65, and the presence of non-malignancy damage were associated with overall cancer risk. For lung cancer (n = 35 cases), smoking was also a prominent risk factor. When looking at haematological cancers specifically (n = 46 cases), there was a suggestion of an increased risk after immunosuppressive drug exposures, particularly when these were lagged by a period of 5 years (adjusted HR 2.29, 95% CI 1.02–5.15).
Conclusions: In our SLE sample, age ⩾65, damage, and tobacco exposure were associated with cancer risk. Though immunosuppressive therapy may not be the principal driving factor for overall cancer risk, it may contribute to an increased risk of haematological malignancies. Future studies are in progress to evaluate independent influence of medication exposures and disease activity on risk of malignancy.
Statistics from Altmetric.com
In many types of systemic autoimmune diseases, including systemic lupus erythaematosus (SLE), there is increasing evidence that cancer (particularly haematological and lung cancers) contributes to both morbidity and mortality.1–4 The most definitive data regarding cancer risk in SLE was generated from our recent large, multi-centre, international cohort study (9547 patients at 23 centres).1 This confirmed a slight increased risk for all cancers combined, and a striking increased risk for haematological malignancies, where the standardised incidence ratio (SIR) estimate was 2.75 (95% CI 2.13–3.49). The data also suggested an increased risk of lung cancer (SIR 1.37, 95% CI 1.05–1.76).
Is this cancer susceptibility caused by immunosuppressive drugs? Despite case reports, data from animal models of lupus,5 and studies of organ transplant recipients,6 7 there is no convincing evidence of this relationship in SLE.8–13 In fact, in our cohort study, the highest SIRs occurred in the first year of SLE duration, suggesting that cancer risk is not completely explained by cumulative exposure to immunosuppressive drugs.
Our objective, therefore, was to determine if, in SLE, exposure to immunosuppressive drugs (specifically cyclophosphamide, azathioprine, and methotrexate) increases the overall risk of cancer. We also performed separate analyses for haematological cancer and for lung cancer, given the particular increased risk of these two cancer types.1 4
METHODS
We conducted a case–cohort study within the previously mentioned multi-site SLE cohort,4 with the participation of 15 collaborating centres in North America, Europe and Asia. These centres represented two research networks, the Systemic Lupus International Collaborating Clinics (SLICC) and the Canadian Network for Improved Outcomes in Systemic Lupus. Included were three centres from Montreal; one centre from each of Toronto, and Calgary; two New York City sites; one centre each from Pittsburgh, Chicago, Baltimore, Chapel Hill North Carolina, and Birmingham Alabama; and one centre each from London, UK, Birmingham, UK, and Seoul, Korea.
We used the case–cohort study design for optimal flexibility and efficiency; in this design, exposure and covariate information is collected from all cases, and a random representative sample of the cohort (“subcohort”; in our case, 10% of the full cohort), which is the source for controls. All of our study subjects were patients with definite SLE (according to American College of Rheumatology (ACR)14 15 or clinical criteria). Cancer cases were ascertained by regional cancer registry linkages. Cases refer to invasive cancers discovered after entry into the lupus cohort at each centre; the index time for each risk (case–control) set was the date of the case’s cancer occurrence. The controls for each risk set, for each cancer case, represented all the subcohort members who remained cancer-free up to that index time.
We used modified Cox proportional hazards regression to calculate the hazard ratio (HR) for cancer after exposure to an immunosuppressive drug, in models that controlled for clinical characteristics, other medication use, tobacco, and demographics, as outlined below. The data on clinical characteristics and all medications were prospectively recorded in the clinic database and/or medical records at each centre, and were then abstracted from these sources using a standardised form. All time-varying variables were treated as time-dependent, assessed for each case–control risk set at the index time.
Immunosuppressive drugs
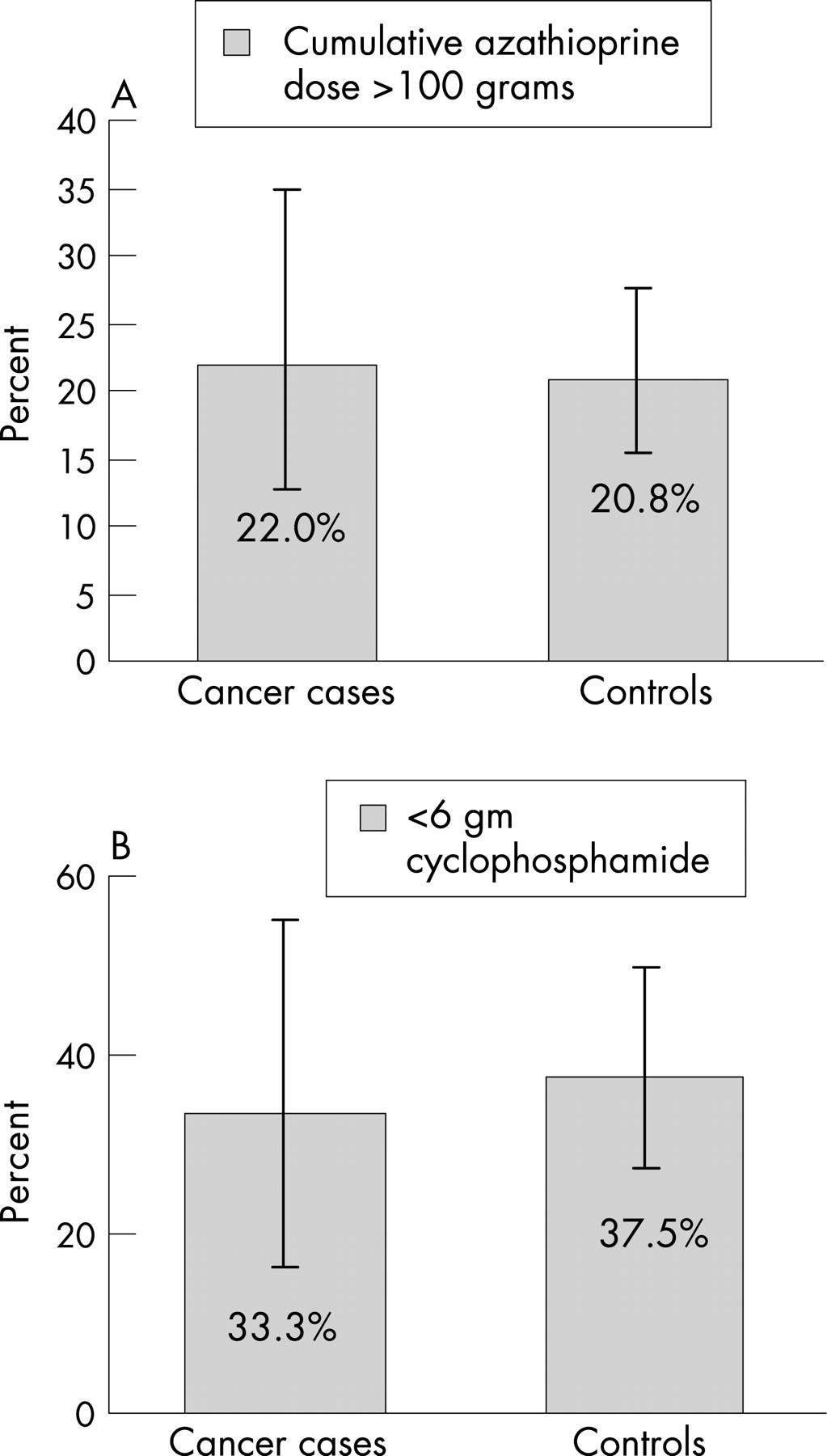
The most common “traditional” immunosuppressive treatment of SLE over our study period (1958–2000) included cyclophosphamide, azathioprine, and methotrexate.16 Thus, we used, as our primary exposure of interest, use of any of these agents from the time of SLE diagnosis up to the time of the index case. Given that some data suggest variable latency periods (ranging from <1 year to >4 years) between exposure and the development of a malignancy,17–19 we considered several exposure windows to cover these possibilities. Separate secondary analyses also considered cumulative exposures for the most common immunosuppressives used in SLE, azathioprine and cyclophosphamide. For azathioprine, we compared, among those exposed to the drug, the percentage of cases vs controls that had been exposed to the equivalent of 100 grams or more. We did the same with cyclophosphamide, considering the exposure of a dose of <6 grams vs higher doses.20–22
Clinical characteristics
As SLE duration may be associated both with the outcome of cancer and with exposure to medications, we controlled for duration of SLE by using this as the time axis, with time zero for each patient being the date of SLE diagnosis, thus matching for disease duration. When point of entry into the cohort was different from time zero, we used left censoring.23 In addition, we controlled for damage scores as assessed by the SLICC/ACR damage index. This is a well-validated, standardised measure capturing total damage from the time of SLE onset onward; damage may be related to SLE activity, treatment or co-morbidities. The index is not a measure of disease activity per se, but has been shown to reflect cumulative disease activity and clinical severity.24–27 The variable for damage in our models was a time-dependent categorical variable capturing whether the patient had sustained any damage up to the index time (not including the damage item related to cancer). Finally, as some have suggested that the association between SLE and lymphoma is mediated through the presence of secondary Sjögren syndrome, in our analyses for haematological cancer, we included a categorical variable indicating physician-confirmed Sjögren syndrome (ie, based on sicca symptoms, anti-Ro/anti-La antibodies, and confirmatory tests, as per diagnostic criteria),28 up to the index time.
Other medication use and tobacco exposure
Non-steroidal anti-inflammatory agents (NSAIDs), including aspirin, may protect against cancer risk;29–32 the effect of glucocorticoids may be complex.33–37 These drugs, along with anti-malarial agents, are often used in SLE, so we adjusted for them in our regression models (time-dependent; categorically (ever/never) in the primary analyses). We also adjusted for tobacco use in our models for its potential effect-modification on our primary exposure of interest.38
Demographics
We adjusted for age, sex, race/ethnicity, calendar year at cohort entry, and geographical residence, using categorical variables for each.
Statistics
To detect possible multicollinearity problems, we examined the data for correlations and associations between independent variables.39
In the hazard regression models, calculation of the parameter variance was performed using methods developed for case–cohort studies, as routine methods do not properly estimate variance.40 41 Separate models were constructed for the outcome of all cancers, haematological cancers only, and lung cancers only. Separate secondary analyses included assessments of the effects of varying lag-times for the drug exposures, and of cumulative doses for cyclophosphamide and azathioprine. To assess the effect of SLE duration on cancer occurrence, we also performed secondary analyses with time since cohort entry as the time scale, with SLE duration considered as a continuous covariate.
RESULTS
Demographics and clinical characteristics appear in table 1. Adjusted HR estimates for our primary analyses are presented in table 2, including 246 cancer cases (46 haematological malignancies and 35 lung cancers) and 538 subjects without cancer. The sample was varied in terms of damage scores, with a range of 0 to 9 (median score 1.0). Missing data regarding damage scores were present in 3.4% of patients; analyses were repeated either leaving out subjects with missing data, or imputing the median value, with similar results. Thus, analyses are presented using the imputed values for these subjects. Missing information on drug exposures was present in 4.9% of subjects. We initially performed the primary analyses excluding these subjects; however, repeating the analyses assuming that most probably subjects had not been exposed, the results were unchanged. Thus, results are presented assuming that these subjects were in fact unexposed. Tobacco exposure included a category for missing data, similar to the approach of others.42 Adjusting for differences in follow-up duration, subjects with a damage score ⩾1 at the end of the observation interval were more likely to have been exposed to prednisone (odds ratio (OR) 2.0, 95% CI 1.4–2.7), or any immunosuppressive (OR 1.7, 1.2, 2.3).
The adjusted HR for overall cancer occurrence after exposure to any immunosuppressive drug (cyclophosphamide, azathioprine, and methotrexate) was 0.82 (95% CI 0.50–1.36). Consideration of drug-specific exposures or lagged exposure times did not alter the results for overall cancer risk appreciably. The multivariate models suggested that cancer risk in SLE was associated with age ⩾65, and the presence of non-malignancy damage as recorded by SLICC/ACR damage scores. For lung cancer, smoking also appeared to be a risk factor (table 2).
In the models for haematological cancer, Sjögren syndrome was not a definite risk factor (table 2, HR 0.96, 95% CI 0.30–3.03). When looking at haematological cancers specifically, there was a suggestion of an increased risk for immunosuppressive drug exposures, best illustrated when immunosuppressant exposures were lagged by 5 year periods (table 3), such that any cancers occurring in the 5 year period immediately after use of an immunosuppressant drug were not attributed to that exposure. This strategy accommodates the latency period that may be present before the effect of these medications on cancer risk is seen. In this model, the adjusted drug-specific HR estimate for haematological cancer after cyclophosphamide exposure was 3.55 (95% CI 0.94–13.37); after azathioprine, 1.02 (95% CI 0.34–3.03); and after methotrexate, 2.57(95% CI 0.80–8.27). As indicated above, an increased risk with latency periods was not seen in the analyses for overall cancer risk.
Examining the data for associations between independent variables, we found only low to moderate correlations between immunosuppressive agents and other medications, and between immunosuppressive agents and other clinical and demographic variables (eg, age); as no correlation coefficients were greater than 0.35, we were reassured regarding the absence of co-linearity.
When we considered dose effects for azathioprine and cyclophosphamide exposures, we saw no clear association of increasing malignancy risk with greater exposure levels (fig 1A,B), although we had limited power to define effects. Similar findings were seen with additional assessments of exposure categories according to duration of exposure (<2 years vs 2–5 years vs >5 years), or for exposure categories of cyclophosphamide comparing <3 gram cumulative exposures vs 3–6 grams vs >6 grams. Most of the cyclophosphamide exposures were intravenous, thus we were unable to reliably differentiate the effect of route (oral vs intravenous) for this drug.

{kind=link}
In sensitivity analyses using time since cohort entry as the time axis, SLE duration was associated with overall cancer risk, with longer duration being protective (adjusted HR 0.88, 95% CI 0.82–0.93).
DISCUSSION
We believe our work has important strengths; the design, a case–cohort study, represents flexible and efficient methodology.41 43–45 Ours is the first major effort to determine if various factors predispose to malignancy in SLE, and offers new insight into what may be driving cancer risk in autoimmune diseases.
One of the difficulties has always been differentiating the effects of medications from disease activity. Adjustment for disease activity is necessary as a potential confounder; however over-adjustment for this variable may diminish the ability to prove effects of drug treatment. In rheumatoid arthritis (RA), another disease with a proven increased risk of haematological (and possibly lung) malignancies,46 the debate has raged for years regarding whether medications or disease activity were more important in driving cancer risk. Very recent work from Baecklund et al has confirmed a very strong association between RA activity and lymphoma.21
The developing story regarding lymphoma and RA activity makes the association in our study between damage scores and cancer all the more interesting. The damage index is not per se a measure of disease activity, but does appear to correlate with cumulative disease activity and clinical severity. Thus, our data may suggest a link between lupus activity and cancer risk. The finding of greatest cancer risk earliest in the course of SLE may also suggest that cancer risk is not completely explained by cumulative exposure to immunosuppressive drugs. However, we are presently embarking on a new study to explore this relationship, with detailed assessments of SLE activity, which should allow us to better delineate effects of this activity vs medication exposures.
Our data did demonstrate an increased risk of lung cancer among smokers with SLE compared to non-smokers. This is, of course, not surprising, as tobacco exposure is a known carcinogen, particularly for lung cancer. There is some evidence in RA18 and other populations38 that the carcinogenic effect of immunosuppressive and cytotoxic medications is heightened by smoking. We did not find definite evidence of such an interaction in our sample (data not shown), but were not able to accurately estimate this potential interaction due to power limitations.
In order to assess global cancer risk, we combined all cancer cases. However the relationship between immunosuppressive drugs might vary considerably with the different type of cancers; in this event, a relatively large increased risk in a rarer cancer types (such as leukaemia and bladder cancer) might be in effect masked if the importance of drug exposures is less important for more common cancer types (such as lung and breast cancer). This emphasises the importance of the separate analyses for haematological cancers. Though the data suggest important findings for this cancer type, we are unable to comment on links between specific immunosuppressive exposures and other cancer types. For example, cyclophosphamide exposure is associated with neoplastic changes in the urinary tract. In our cohort study of malignancy risk in SLE, we had observed only 13 bladder cancers over 76 948 patient-years of follow-up. Although not precise enough to definitively state the magnitude of a potentially increased bladder cancer risk in SLE, the point estimate from that study suggested an increase of about 25% from the expected rate (SIR 1.23, 95% CI 0.66–2.11). Given this, we continue to advocate measures to decrease potential risk associated with this agent, by ensuring good hydration, by administration of intravenous cyclophosphamide with 2-mercaptoethane sodium sulfonate (MESNA, which binds toxic metabolites), and by limiting cumulative exposures where possible. Patients with a history of cyclophophamide exposure should be subjected to life-long periodic monitoring of urine cytology to detect occult malignancy, and other investigations (ie, cystoscopy) as required.
Similarly, a link between immunosuppressive and cervical dysplasia has been recorded in the literature, and appears to be greatest for cyclophosphamide.47 However, our cohort study focused on invasive cancers, as data on precancerous lesions such as cervical dysplasia are generally not available from tumour registries. Thus, we could not estimate, in the current analyses, the effects of immunosuppressives on cervical dysplasia. However, other data that we have published certainly do substantiate that immunosuppressive agents increase risk of cervical dysplasia,48 likely due to impeded clearance of human papilloma virus (HPV) infection.49 This makes it imperative that women exposed to immunosuppressive agents undergo regular screening for cervical dysplasia, as per current guidelines.50
Regarding other limitations of our work, in our primary analyses we adjusted simply with categorical variables, for ever/never exposures. This was, we felt, an acceptable primary approach as we had this level of detail on all subjects, and for most variables we were chiefly interested in potential effect-modification of our primary exposure of interest.38 However, our exploratory analyses considered alternate definitions (including cumulative exposures). Additionally, although we had collected exposure information for our subjects on immunosuppressive drugs other than cyclosphosphamide, azathioprine, and methotrexate, these were not of sufficient frequency to allow individual analyses. (Mycophenolate exposure, for example, occurred in only 3.6% of subjects, as it has been introduced only relatively recently.) Regardless, including all of these agents as part of the ever/never immunosuppressive drug exposure variable did not alter our results appreciably. Finally, even though ours is the largest relevant study to date, we unfortunately did not have the power to allow us to test for interactions between multiple exposures, or between immunosuppressive treatment and factors such as age and calendar year. Power limitations may also have prevented us from distinguishing dose-related effects in our current study, particularly in the exploratory analyses that examined different exposure time windows.
In the oncology literature concerning risk of second cancers after alkylating agent therapy, increasing cumulative dose or duration of treatment with cyclophosphamide was not clearly associated with increasing risk.51 52 In RA, there have been a handful of controlled studies assessing cyclophosphamide and azathioprine use and malignancy risk. Asten et al assessed cumulative exposures in a large cohort of rheumatic disease patients and found a positive relationship between duration of exposure and malignancy risk (for haematological, skin, and bladder cancers); however, disease severity was not controlled for.22 Other studies have suggested a role for cumulative drug dose/duration in RA, particularly regarding cyclophosphamide.18 53 One important issue is that exposure to this agent is likely more linked to leukaemia, than lymphoma. Thus, some haematological malignancies in autoimmune diseases may be caused by drugs; however, for lymphoma risk, disease activity may be equally important.
Our inability to illustrate a role for cumulative drug dose/duration in our own sample may also reflect different dosing schedules for RA vs SLE. In RA, oral cyclophosphamide had been prescribed at a dose of up to 2.5 mg/kg/day; in the study of Baker et al,53 the mean duration of cyclophosphamide exposure was 43.8 months and the mean total dose was about 75 grams. In contrast, in SLE, the agent is most often given in intravenous pulses at 1–3 monthly intervals, for a duration of 6 to 24 months, or a total of about 6–12 grams (albeit repeated courses are sometimes required).
More recently, in Baecklund et al’s work showing an association of lymphoma with azathioprine use in RA, controlled for disease activity,21 there was no clear evidence of increasing risk with therapy duration.
Though cancer risk is increased in SLE, haematological malignancies remain a relatively uncommon event, with less than one event occurring per 1000 patient-years.1 4 Additionally, the same drugs that may have adverse consequences in terms of cancer risk, may have beneficial effects in terms of control of SLE disease and prevention of other long-term sequelae (such as renal dysfunction); this risk: benefit ratio must be kept in mind.
In summary, we have estimated cancer risk after exposure to immunosuppressive agents in SLE. Though immunosuppressive therapy may not be the primary driving factor for malignancy occurrence overall, it appears to contribute to haematological malignancy risk. Our results set the stage for future evaluations of long-term effects of emerging agents.
Acknowledgments
Gina Banks functioned as the research co-coordinator responsible for all US sites. We wish to thank Dr Simon Bowman, Dr Deva Situnayake, and Dr Veronica Toescu for their significant contributions in providing patient access and the collection of data for the Birmingham UK cohort. Dr Martha Sanchez at the University of Alabama, Birmingham assisted with data collection for the UAB SLE cohort. Research associates Stephanie Heaton (Birmingham UK), Whitney Steber (Calgary) and Anne McKinnon (Toronto) assisted greatly with data collection at these centres. We would like to acknowledge the following tumour registries, which performed the linkage studies: the Quebec Tumour Registry, Cancer Care Ontario, Alberta Tumour Registry, Illinois State Cancer Registry, Maryland Cancer Registry, University of North Carolina Cancer Registry, New York State Tumor Registry, Pennsylvania Cancer Incidence Registry, Alabama Cancer registry, Thames Cancer Registry, British West Midlands Cancer Registry, and the National Statistical Office in Korea. The Pennsylvania Department of Health requested a disclaimer for any responsibility on their part for any analyses, interpretations or conclusions. We also thank the regional and national vital statistics registries for providing vital status information on deceased and lost to follow-up subjects.
REFERENCES
Footnotes
-
Funding: SB was sponsored by the Canadian Institutes of Health Research (CIHR) Junior Investigator Award; Fonds de la Recherche en Santé du Québec (FRSQ); Lupus Canada Fellowship; and Canadian Arthritis Network Scholar Award. LJ was sponsored by a CIHR Senior Investigator Award. PRF was sponsored by Arthritis Centre of Excellence University of Toronto, Arthritis & Autoimmunity Research Centre, University Health Network, Lupus Canada; and Investigator Award The Arthritis Society (TAS)/CIHR. MP was sponsored by The Hopkins Lupus Cohort supported by NIH AR437337 and the Johns Hopkins University Clinical Research Centre M01-RR00052. GSA was sponsored by NIAMS P01AR49084 and GCRC M01-RR00032 (UAB). CG was sponsored by financial support for the Birmingham UK lupus cohort provided by Lupus UK. J-LS was sponsored by CIHR MOP-62687. AC was sponsored by the Singer Family Fund for Lupus Research; FRSQ National Scholar Award; TAS 99-105; CIHR MOP-57816, MOP-62817, MOP-74630; and National Cancer Institute of Canada 013135. RR-G was sponsored by the Arthritis Foundation, Clinical Science Grant, Arthritis Foundation Greater Chicago Chapter NIH RO-3 CA 110904, AR 02138, AR 48098; and Lupus Foundation of Illinois Chapter Grant.
-
Competing interests: None