Article Text

Abstract
Objectives To determine the frequency, accrual, attribution and outcome of neuropsychiatric (NP) events and impact on quality of life over 3 years in a large inception cohort of patients with systemic lupus erythematosus (SLE).
Methods The study was conducted by the Systemic Lupus International Collaborating Clinics. Patients were enrolled within 15 months of SLE diagnosis. NP events were identified using the American College of Rheumatology case definitions, and decision rules were derived to determine the proportion of NP disease attributable to SLE. The outcome of NP events was recorded and patient-perceived impact determined by the SF-36.
Results 1206 patients (89.6% female) with a mean (±SD) age of 34.5±13.2 years were included in the study. The mean disease duration at enrolment was 5.4±4.2 months. Over a mean follow-up of 1.9±1.2 years, 486/1206 (40.3%) patients had ≥1 NP events, which were attributed to SLE in 13.0–23.6% of patients using two a priori decision rules. The frequency of individual NP events varied from 47.1% (headache) to 0% (myasthenia gravis). The outcome was significantly better for those NP events attributed to SLE, especially if they occurred within 1.5 years of the diagnosis of SLE. Patients with NP events, regardless of attribution, had significantly lower summary scores for both mental and physical health over the study.
Conclusions NP events in patients with SLE are of variable frequency, most commonly present early in the disease course and adversely impact patients' quality of life over time. Events attributed to non-SLE causes are more common than those due to SLE, although the latter have a more favourable outcome.
Statistics from Altmetric.com
Introduction
The frequency of neuropsychiatric (NP) disease in systemic lupus erythematosus (SLE) varies between 37% and 95%.1,–,5 Differences in the definition and ascertainment of NP manifestations, lack of consistency in the attribution of NP events and inclusion of subtle NP disease of uncertain clinical significance contribute to this variability. The fluctuating course of many NP manifestations emphasises the need to evaluate their impact over time.
An international, multicentre, prospective, inception cohort study of NP events in patients with SLE was undertaken using uniform definitions and decision rules for determination of attribution. We previously reported on NP events at enrolment,6 including short-term outcome over a mean of 3.7 months. In this study, we report the clinical characteristics, outcome and impact on health-related quality of life (HRQoL) in an expanded cohort of patients evaluated over 3 years and up to four annual assessments with a mean follow-up of 23 months.
Patients and methods
Research network
The study was performed by the Systemic Lupus International Collaborating Clinics (SLICC)7 between October 1999 and February 2008 and was approved by the Capital Health Research Ethics Board, Halifax, Nova Scotia, Canada and by the institutional research ethics boards of participating centres.
Patients
Patients fulfilled the American College of Rheumatology (ACR) classification criteria for SLE8 and provided written informed consent. The date of diagnosis was taken as the point at which four or more ACR criteria were first recognised, and enrolment occurred up to 15 months after the diagnosis. Patients were reviewed at enrolment and annually (±6 months) thereafter when new NP events since the previous visit and the status of old events were recorded. Other data included age, gender, ethnicity, education, medication use, SLE Disease Activity Index (SLEDAI)9 and SLICC/ACR Damage Index (SDI).10 HRQoL was measured by the SF-36.11 Laboratory data included a complete blood count, serum creatinine, urine analysis, anti-DNA, C3 and C4.
Neuropsychiatric events
All NP events were characterised using the ACR case definitions and were diagnosed by clinical evaluation supported with appropriate investigations according to the ACR glossary12 (see online supplementary file #1). The exception was cognitive impairment, for which the diagnosis was made by formal neuropsychological testing in only 9/43 (21%) cases.
Outcome of NP events
A doctor-generated seven-point Likert scale compared the change in NP status between the onset of the event and time of study assessment (1=patient demise, 2=much worse, 3=worse, 4=no change, 5=improved, 6=much improved, 7=resolved). The time to resolution was the interval between the onset of the event and the date of resolution; if the NP event had not resolved, the time was censored to onset of the event and the date of the final assessment. Analyses of both time to resolution and Likert outcome scores were undertaken. A patient-generated mental (MCS) and physical (PCS) component summary score of the SF-3611 determined the impact of NP events on HRQoL.
Statistical analysis
NP events were attributed to SLE or non-SLE causes (see online supplementary file #1) and categorised into central/peripheral and diffuse/focal nervous system manifestations as described6 12 (see supplementary file #2). SLICC centres were grouped into geographical locations (Canada, USA/Mexico, Europe, Asia). For some analyses patients were categorised at each assessment as NP positive with (A) diffuse/central events only; (B) focal/peripheral events only; (C) both events and (D) an NP negative group.
χ2 and t tests examined differences in demographics and NP status at enrolment between patients with missing data and patients who completed the study. Explanatory variables for time-to-case resolution for NP events were examined using Cox regression (adjusting for correlation of events in the same patient).
Likert outcome scores of NP events were analysed using multilevel ordinal logistic regression, with odds ratios linked to the probability of higher, more favourable, scores, and accounting for correlation of multiple scores over time for the same event and multiple events for the same patient. SF-36 analyses used linear regression and generalised estimating equations with a first-order autoregressive correlation structure to allow for correlation between multiple SF-36 measurements for the same patient.
Results
Patients
A total of 1206 patients were recruited in 24 centres. Patients were predominantly female (89.6%) and Caucasian with a mean±SD age of 34.5±13.2 years (table 1).
Demographic and clinical manifestations of patients with systemic lupus erythematosus (SLE) at enrolment visit
The mean disease duration was 5.4±4.2 months in an unselected patient population with moderate disease activity. The mean follow-up for NP events (the onset of NP events to the last assessment) was 1.9±1.2 years. No follow-up was available in 191/1206 (15.8%) patients and the assessment for the last expected date plus 6 months was unavailable in 353/1206 (29.3%). These patients were more likely to be younger (p<0.008), Hispanic or Black (p<0.0001), had less education (p<0.006) and higher SLEDAI scores (6.1±6.3 vs 5.2±5.2; p<0.023). They were also less likely to have NP disease, attributed to SLE or non-SLE causes, at the enrolment assessment (p<0.023). There were 18/1206 (1.5%) deaths and in 4/18 (22.2%) cases the primary cause was attributed to NP events (intracranial haemorrhage (two), stroke (one), seizures (one)).
Frequency and attribution of NP events
Four hundred and eighty-six of 1206 (40.3%) patients had at least one NP event during the study; 210 (17.4%) had two or more events. The 486 patients had 843 events encompassing 18/19 NP syndromes (table 2).
The number of neuropsychiatric (NP) events by attribution over the period of study
The most common events were headache (migraine (49%), tension (38%), intractable 9%, cluster (3%), pseudotumour cerebri (1%)), mood disorders, seizures, cognitive dysfunction, anxiety disorder, cerebrovascular disease, acute confusional state, polyneuropathy and mononeuropathy. The remaining 10 NP syndromes had a prevalence of <2%; myasthenia gravis did not occur in any patient.
NP events attributed to SLE varied from 17.7% (model A) to 30.6% (model B) (table 2). Of the 843 NP events, 785 (93.1%) affected the central nervous system and 58 (6.9%) involved the peripheral nervous system. Diffuse and focal events were 666 (79%) and 177 (21%), respectively. The most common NP events attributed to SLE were seizures, mood disorders, cerebrovascular disease and acute confusional states.
Onset and accrual of NP events
NP events were most common at the enrolment visit and the cumulative incidence of both SLE and non-SLE NP events increased over time (figure 1). Of patients with follow-up to the final study assessment, 51.2% had at least one NP event. The proportion of patients with NP events attributed to SLE varied between 13.0% (model A) and 23.6% (model B). The proportion of patients with both SLE and non-SLE attributed NP events was 7.9% (model A) and 14.2% (model B).

The cumulative frequency of patients with neuropsychiatric (NP) events at enrolment and at subsequent study assessments. The percentage of patients with NP events is shown at each time point for all NP events regardless of attribution (all NP), NP events attributed to non-systemic lupus erythematosus (SLE) causes (non-SLE NP), NP events attributed to SLE according to attribution model B (SLE NP (B)) and NP events attributed to SLE according to attribution model A (SLE NP (A)).
Outcome of NP events
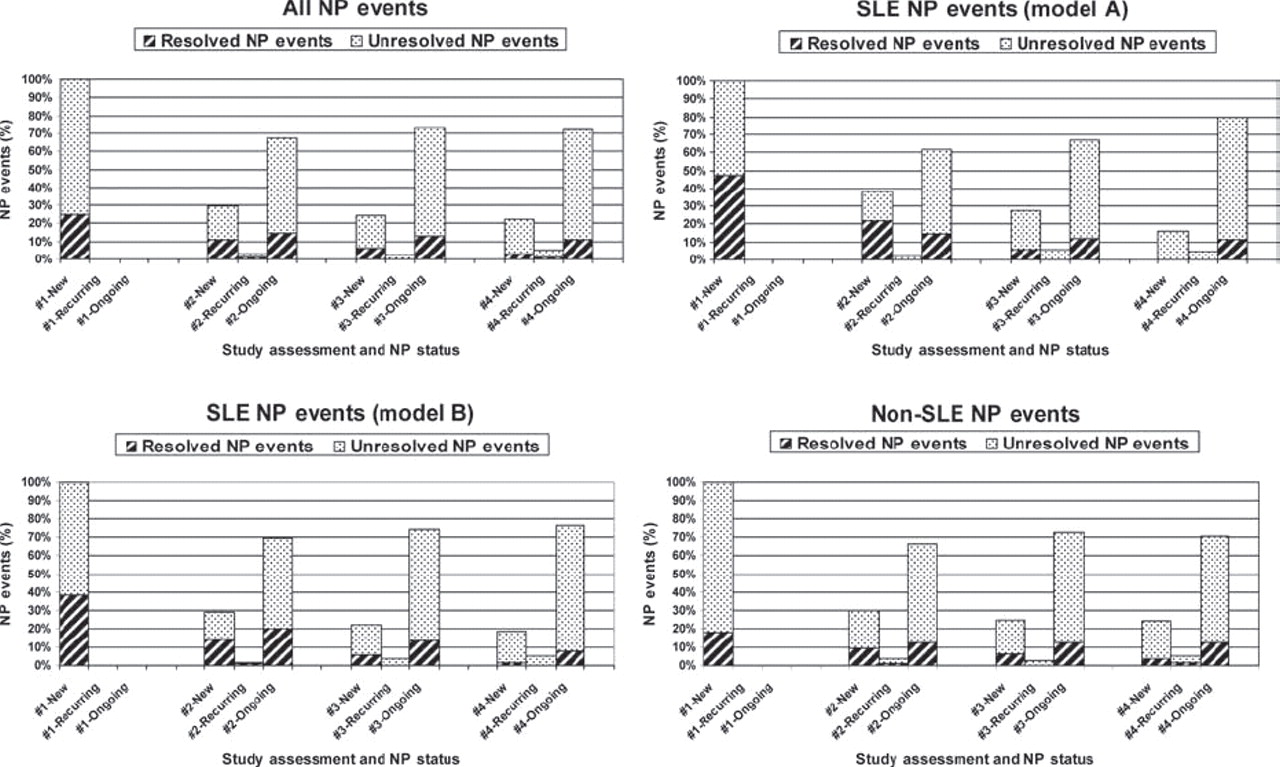
There was no difference in the attribution frequency of new, recurring or ongoing NP events (figure 2). However, the rate of resolution of NP events attributed to SLE was higher than events due to non-SLE causes (model A: 55.0% vs 38.2%, hazard ratio (HR)=1.62, 95% CI 1.24 to 2.11, p<0.001; model B: 51.9% vs 36.4%, HR=1.53, 95% CI 1.22 to 1.92, p<0.001). There was a higher resolution of focal versus diffuse NP events (52.5% vs 38.1%, HR=1.55, 95% CI1.21 to 1.98, p<0.001) but no difference between the resolution of central versus peripheral NP events (41.4% vs 37.9%, HR=1.23, 95% CI 0.79 to 1.93, p=0.358).

The frequency of neuropsychiatric (NP) events at enrolment and at subsequent study assessments characterised as new, recurring or ongoing from a previous assessment. At each assessment the status of the NP events into resolved or unresolved is shown. Summary data are shown for NP events regardless of attribution (all NP events), NP events attributed to systemic lupus erythematosus (SLE) according to attribution model A (SLE NP (model A)), NP events attributed to SLE according to attribution model B (SLE NP (model B)) and NP events attributed to non-SLE causes (non-SLE NP).
To look for an interaction between disease duration and the effect of attribution on NP event resolution, disease duration at the occurrence of events was dichotomised at 1.5 years. For model A the estimated SLE attribution effect on resolution of events within 1.5 years of the diagnosis of SLE was larger than the effect for events occurring ≥1.5 years after the diagnosis (HR=1.77 vs 0.89) (interaction coefficient=−0.69, 95% CI −1.52 to 0.15, p=0.107). For model B, the same analysis led to a hazard ratio comparison of: 1.66 vs 0.86 (interaction coefficient=−0.66, 95% CI −1.39 to 0.07, p=0.076).
Favourable Likert outcome scores for NP events were more common for those attributed to SLE (model A or model B), particularly at the first two study assessments (figure 3). Controlling for the duration of follow-up, multivariate ordinal regression analysis confirmed a significant positive association between favourable outcome scores and SLE NP events (model B) (odds ratio (OR)=1.51, 95% CI 1.05 to 2.21, p=0.028), focal NP events (OR=1.83, 95% CI 1.28 to 2.64, p=0.001), US/Mexico (OR=1.32, 95% CI 0.90 to 1.93), European (OR=1.66, 95% CI 1.12 to 2.46) and Asian (OR=2.79, 95% CI 1.41 to 5.50) sites (p=0.007), and negative associations with older age at SLE diagnosis (OR=0.69, 95% CI 0.59 to 0.81), p<0.001), longer disease duration at event onset (OR=0.79, 95% CI 0.69 0.90), p=0.001) and higher SLEDAI scores computed without NP variables (OR=0.95, 95% CI 0.93 to 0.98), p=0.002), all of which were included in the models as continuous variables. The interaction between disease duration at event onset and attribution of an NP event was again only marginally significant (p=0.095).
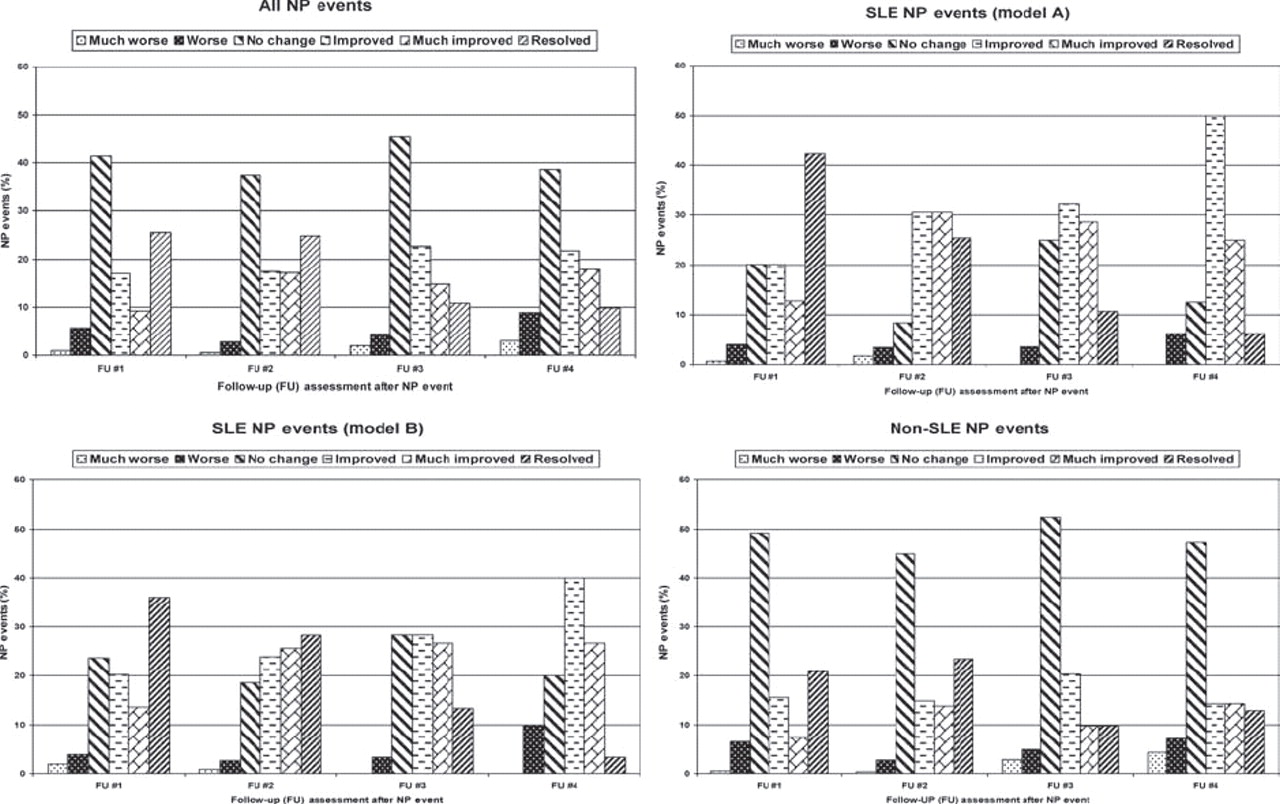
The outcome of neuropsychiatric (NP) events over the duration of the study. Events are clustered into all NP events regardless of attribution (all NP events), NP events attributed to systemic lupus erythematosus (SLE) according to attribution model A (SLE NP events (model A)), NP events attributed to SLE according to attribution model B (SLE NP events (model B)) and NP events attributed to non-SLE causes (non-SLE NP events). Within each panel the outcome of the events is scored as much worse, worse, no change, improved, much improved and resolved at assessments 1 through 4 compared with the onset of the event.
NP events and HRQoL
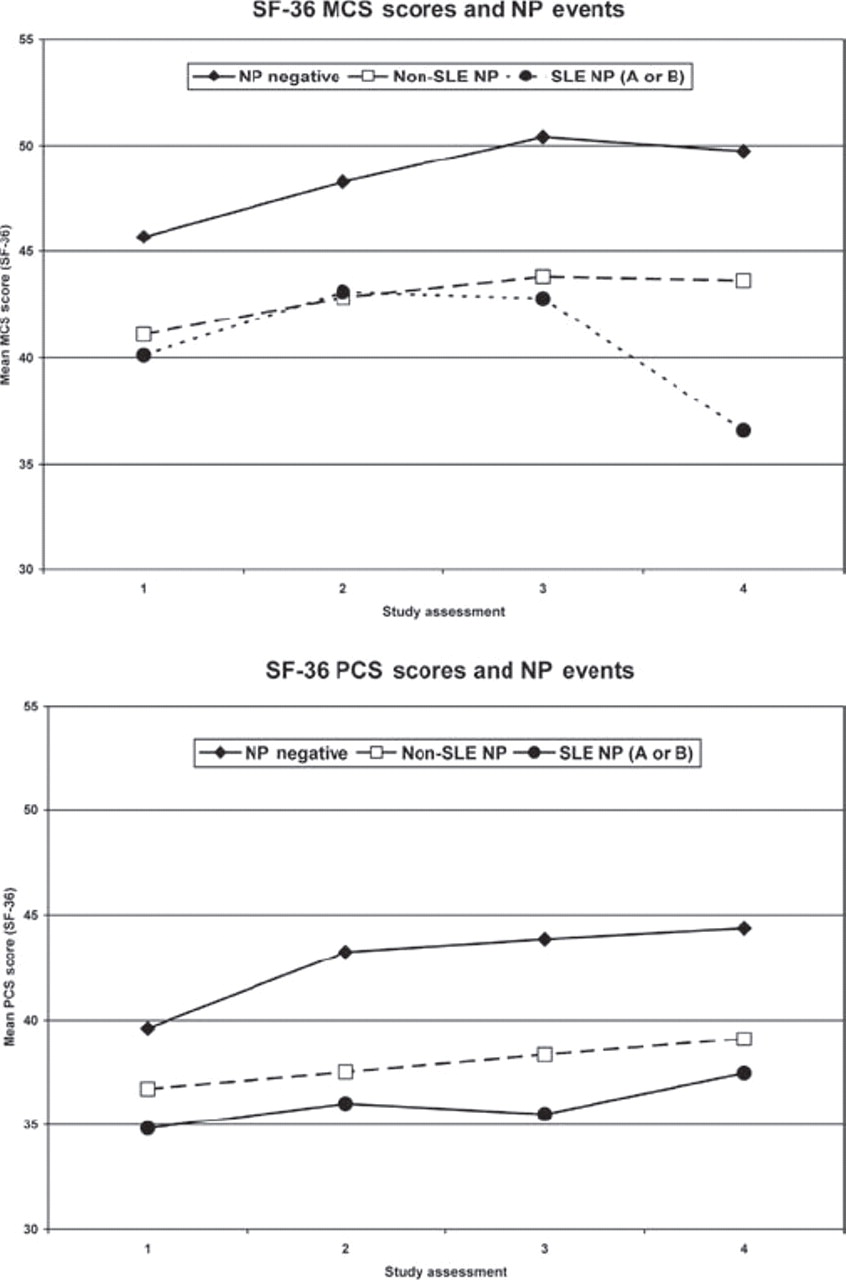
In a multivariate regression analysis there were significantly lower MCS scores in patients with NP events regardless of attribution than in those without events (estimate: −9.7, 95% CI −12.7 to −6.7; p<0.001) (figure 4). Controlling for gender, age at SLE diagnosis, disease duration at each visit, a summary multivariate analysis also demonstrated associations between lower MCS scores and diffuse NP events (eg, patients with diffuse vs focal NP events only: estimate=−5.0, 95% CI −9.2 to −0.8; global p=0.041); higher SLEDAI scores (estimate: −0.15, 95% CI −0.30 to −0.01, p=0.041) and higher SDI scores, both computed without NP variables (eg, SDI >3 vs ≤3: estimate=−5.7, 95% CI −10.4 to −0.9; global p=0.039).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean mental component summary (MCS) score and physical component summary (PCS) score of the Short Form-36 (SF-36) over the period of study in patients with no NP events (NP negative), NP events attributed to non-systemic lupus erythematosus (SLE) causes (non-SLE NP) and NP events attributed to SLE according to attribution model A or B (SLE NP A or B) at each of the study assessments. (See supplementary fi le #3)
Similarly, the group means for the PCS scores were significantly lower in patients with NP events (estimate: −3.3, 95% CI −4.5 to −2.1, p<0.001) regardless of attribution (figure 4). In a summary multivariate analysis controlling for ethnicity, age at SLE diagnosis and disease duration at each visit, other significant associations with lower PCS scores were with study sites (eg, US/Mexico vs rest: estimate: −5.3, 95% CI −7.2 to −3.4; global p<0.001); female gender (estimate: −2.3, 95% CI −4.3 to −0.3, p=0.024); lack of college education (estimate: −2.7, 95% CI −4.1 to −1.3, p<0.001); higher SLEDAI scores (estimate: −0.35, 95% CI −0.48 to −0.22, p<0.001) and higher SDI scores (eg, SDI >3 vs ≤3: estimate: −5.2, 95% CI −8.9 to −1.5; global p<0.001) computed without NP variables.
Discussion
We have established a large, SLE disease inception cohort for the systematic evaluation of NP events in a long-term prospective study. A unique feature of the study is inclusion of all NP events regardless of their aetiology, so that differences in the outcome and impact of NP events due to SLE and other causes could be compared. Attribution of NP events was determined using predefined decision rules which have previously provided a positive correlation between SLE NP events and pathogenic autoantibodies.13 Over the study, 40.3% of patients had at least one NP event and 17.4% had multiple events. However, patients with NP events attributed to SLE varied from 13.0% to 23.6%, depending upon the stringency of the attribution rules. Likewise, only 17.7% to 30.6% of all NP events were attributed to SLE. Finally, many of the 19 syndromes occurred in <2% of patients, indicating that they are relatively infrequent, at least in the first 3 years of the disease.
The outcome of NP events in patients with SLE, particularly those attributed directly to SLE, has been informed by clinical trials,14,–,19 retrospective and prospective observational cohorts and case series,20 21 with inconsistent results. In this study the most favourable outcomes occurred with NP events attributed to SLE compared with non-SLE causes and with focal NP compared with diffuse NP events. Furthermore, the outcome was best in SLE-attributed events when they occurred early in the disease course, suggesting that the attribution and time of onset of NP events predict outcome. As for rheumatoid arthritis22 23 this may indicate a therapeutic window of opportunity when pathogenetic mediators are amenable to immunosuppressive and anti-inflammatory treatments. This study confirms and expands the findings of previous cross-sectional studies reporting that NP events, regardless of attribution, are associated with a significant reduction in patient self-reported HRQoL.3 24 25 Thus, in addition to lower group means for MCS and PCS scores of the SF-36 in patients with NP events compared with those without NP events at enrolment, the same group differences persist over the ensuing 3 years. Our results also emphasise the importance of assessing the impact of all NP manifestations, as studies confined to specific subsets of NP disease such as cognitive dysfunction have not found a negative effect on HRQoL.26 27
There are potential limitations to our study. First, the frequency of patients with unavailable data (29%) or no follow-up (15.8%) by the final study assessment is high compared with some longitudinal lupus cohorts with rates as low as 11%.28 29 However, these cohorts were more homogeneous and followed up at single centres. In contrast, 29% lost to follow-up over 3.5 years was reported in a large, multiethnic, multicentre cohort with very similar predictors as in our study.30 Second, restricting NP syndromes to the 19 ACR case definitions12 might have excluded some NP presentations. However, none of the 1206 patients had an NP event which could not be captured within the ACR definitions. Finally, formal neuropsychological assessments were not performed on all patients and neuroimaging studies were only done if clinically indicated. Although additional abnormalities would probably have been detected by both techniques, our protocol was intended to reflect clinical practice and to avoid the inclusion of subtle NP disease with limited clinical significance.26 31,–,36
In summary our findings indicate a high cumulative frequency of NP events and a negative impact on HRQoL, even though the majority of NP events are not attributable to SLE. Those events attributed to SLE and focal NP events have a better outcome. Future studies will examine the long-term course and impact of nervous system disease and search for biomarkers and pathogenic mechanisms of NP events in this unique cohort of patients with SLE.
Acknowledgments
We are grateful for the generous donation of our patients' time and the dedication of all the research coordinators and research assistants in the SLICC network to the completion of this work. In addition, the contribution of Dr Hwee-Cheng Chong at the University of Birmingham, Birmingham, UK, is greatly appreciated.
References
Supplementary materials
Web Only Data ard.2008.106351
Files in this Data Supplement:
Footnotes
-
Funding JGH (Canadian Institutes of Health Research grant MOP-57752, Capital Health Research Fund); MBU (Canadian Institutes of Health Research grant MOP-49529, Lupus Foundation of Ontario, Ontario Lupus Association, Lupus UK, Lupus Foundation of America, Lupus Alliance Western New York, Conn Smythe Foundation, Tolfo Family (Toronto); LS (MRC (UK) grant U.1052.00.009); SCB (Korea Healthcare technology R & D project, Ministry for Health, Welfare and Family Affairs, Republic of Korea (A080588)); CG (Lupus UK, Arthritis Research Campaign, Wellcome Trust Clinical Research Facility in Birmingham, UK); AC (Fonds de la recherche en santé de Quebec National Scholar, Singer Family Fund for Lupus Research); SB (Canadian Institutes of Health Research Junior Investigator Award; Fonds de la recherche en santé du Québéc Jeune Chercheure; Canadian Arthritis Network Scholar Award; McGill University Health Centre Research Institute); GSA (University of Alabama at Birmingham, grant P60AR48095); DDG (Canadian Institutes of Health Research); PRF (distinguished senior research investigator of the Arthritis Society and Arthritis Centre of Excellence); MP (Hopkins Lupus Cohort grant AR 43727, Johns Hopkins University General Clinical Research Center grant MO1 RR00052); SM(National Institutes of Health research grants R01 AR46588, K24 AR002213 and M01 RR000056); RR-G (National Institutes of Health research grants M01-RR00048; K24 AR02318; P60 AR 48098); ON (Swedish Medical Research council grant 13489); GS (Swedish Medical Research council grant 13489); VF (MRC(UK) grant U.1052.00.009).
-
Competing interests None.
-
Ethics approval This study was conducted with the approval of the Capital Health Research Ethics Board, Halifax, Nova Scotia, Canada and by the institutional research ethics boards of participating centres in accordance with the Declaration of Helsinki's guidelines for research in humans.
-
Provenance and peer review Not commissioned; externally peer reviewed.