Article Text

Abstract
Objective To investigate whether the risk allele for systemic lupus erythematosus (SLE) in the signal transducer and activator of transcription factor 4 (STAT4) gene, defined by the single nucleotide polymorphism (SNP) rs10181656(G), is associated with vascular events and/or presence of prothrombotic anti-phospholipid antibodies (aPL) in patients with SLE.
Methods Two independent groups of unrelated patients with SLE of Swedish ethnicity (n=424 and 154) were genotyped, and occurrence of previous manifestations of ischaemic heart disease (IHD), ischaemic cerebrovascular disease (ICVD) and venous thromboembolic events (VTE) was tabulated. aPL values were measured by ELISA. Matched controls (n=492 and 194) were genotyped.
Results The STAT4 risk allele was more frequent in patients with SLE with previous arterial events (combined OR (ORc)=1.5, 95% CI 1.1 to 2.0) compared to patients without such events. The association was mainly attributable to an accumulation of the risk allele among patients with ICVD (ORc=2.3, CI 1.6 to 3.3). There was no association with IHD or VTE. The presence of two or more aPLs was associated with the risk allele (ORc=1.6, 95% CI 1.2 to 2.0). In multivariable-adjusted logistic regression analyses treatment for hypertension, at least one STAT4 risk allele, older age, IgG anti-cardiolipin antibodies and longer SLE duration remained independently associated with previous ICVD (p≤0.02 for all).
Conclusion Patients with SLE with the STAT4 risk allele had a strikingly increased risk of ICVD, comparable in magnitude to that of hypertension. The results imply that a genetic predisposition is an important and previously unrecognised risk factor for ICVD in SLE, and that aPLs may be one underlying mechanism.
Statistics from Altmetric.com
Introduction
While survival in general in systemic lupus erythematosus (SLE) has improved a marked increased incidence of cardiovascular disease (CVD) has become more apparent.1 2 The rate of death from CVD was estimated to be three times higher in patients with SLE than in the general population. Mortality due to coronary heart disease and stroke was increased, and vascular mortality seemed to have remained constant since 1964.3
Several traditional CVD risk factors are prevalent in patients with SLE, but they do not fully account for the high incidence of CVD.4 Additionally, SLE-related factors, for example, anti-phospholipid antibodies (aPL) and proinflammatory biomarkers seem to be important.5,–,7 A genetic deficiency of mannose-binding lectin8 9 and a polymorphic GT repeat in the C reactive protein (CRP) gene (CRP GT20)10 were previously reported to be associated with arterial events in SLE. However, no study has evaluated the association between CVD in SLE and the common susceptibility genes for this disease, recently identified in whole genome association studies.11 12
The signal transducer and activator of transcription factor 4 (STAT4) has reliably been demonstrated to be one of the strongest genetic susceptibility factors for SLE. The STAT4 risk alleles is associated with a more severe SLE phenotype characterised by younger age at disease onset, higher frequency of nephritis and presence of anti-double stranded DNA antibodies.11,–,17
STAT4 transmits signals from the receptors for type I interferon (IFN), interleukin 12 (IL12) and IL23 and it appears to be a critical mediator for several proinflammatory cytokines and chemokines including IFNα.18 Increased production of IFNα, present in a majority of patients with SLE19 may contribute to vascular vulnerability in SLE through amplifying inflammatory activity in atherosclerotic plaques and may also impair endothelial progenitor cell differentiation.20
We have previously investigated a set of 53 common single nucleotide polymorphisms (SNPs) in the STAT4 gene. Of these SNPs, 10 were associated with SLE.17 The strongest signal of association was observed for two perfectly linked STAT4 SNPs, rs10181656 and rs7582694 (r2=1.0), which are in perfect linkage disequilibrium with the SNP rs7574865, also shown to be associated with SLE.21 Either one of these SNPs accounted for the entire observed association signal in our study.17 We therefore used the SNP rs10181656(G) as a representative of the STAT4 SLE risk allele and investigated its association with vascular manifestations and presence of prothrombotic aPL in two independent SLE groups.
Methods
Study population
Two patient groups with SLE were included. The first group was from the rheumatology clinics at Karolinska and Uppsala University hospitals (mid Sweden, n=443). The second group was from Lund University hospital (southern Sweden, n=154). All patients attending the respective hospitals were invited to participate. If patients were related only the first case in each family was included; thus the study population included unrelated patients. A rheumatologist examined all patients and their medical records. All patients fulfilled at least four of the American College of Rheumatology (ACR) classification criteria for SLE.22 Organ damage was estimated using the Systemic Lupus International Collaborating Clinics (SLICC)/ACR damage index.23 The regional ethical boards approved the study. All study participants gave informed consent to participate. We explored risk allele frequencies in subgroups of patients with SLE as defined by the occurrence of previous vascular events or a positive test for aPL of different specificities.
Matched controls were genotyped to give a comparison to the local genetic background. Control samples from mid Sweden were from healthy blood donors (n=153) or from population-based individuals (n=309) matched for age, sex, ethnicity and region of living. Control samples from southern Sweden (n=194) were from healthy blood donors matched for ethnicity and region of living. Standard procedures were used to extract DNA from blood samples.
Outcomes
Vascular events were objectively verified (see supplementary material for detailed definitions) (NB for ‘any arterial event’, we refer to the occurrence of one or more of events 1–3):
Ischaemic heart disease (IHD): myocardial infarction (MI) and/or angina pectoris.
Ischaemic cerebrovascular disease (ICVD): ischaemic stroke and/or transitory ischaemic attacks (TIA).
Ischaemic peripheral vascular disease (IPVD): intermittent claudication and/or peripheral arterial thrombosis or embolus.
Venous thromboembolism (VTE): deep vein thrombosis and/or pulmonary embolism.
Antibodies and lupus anticoagulant
Antibodies against (1) cardiolipin (CL, IgG and IgM), β2 glycoprotein 1 (βGP-1, IgG) and prothrombin (PT, IgG) were successfully analysed by ELISA (Orgentec, Mainz, Germany) in >99% of frozen serum samples. The cut-off levels corresponded to the 99th percentile of healthy blood donors. Lupus anticoagulant (LAC) was determined with a modified dilute Russel viper venom method, (Biopool, Umeå, Sweden) using Bioclot lupus anticoagulant.
Genotyping
The SNP rs10181656 in intron 3 of the STAT4 gene was genotyped using the Golden Gate assay (Illumina, San Diego, California, USA)24 in 497 patients with SLE and 536 controls from mid and southern Sweden as previously described and presented.17 The genotype call rate was 97.0% and the reproducibility 100% as determined by duplicate genotyping of 17 samples. An additional, partly overlapping, set of 417 participants was genotyped using the SNPstream system (Beckman-Coulter, Fullerton, California, USA). This method uses PCR amplification followed by single-base primer extension with fluorescent ddNTPs.25 The sequence of the forward PCR primer was 5′-TGGGAAAATAGTTTTCAAAGTCTAA-3′ and that of the reverse primer was 5′-AAGATGGTGACAAGCCAGG-3′ and the sequence of the detection primer was 5′-ACTAGCTGGAATCCAACTCTTCTCA-3′. For this assay the genotype call rate was 97.6% and the reproducibility 100% as determined by duplicate genotyping of 191 samples. For the overlapping set of 156 individuals successfully genotyped by both assays the concordance between platforms was 100%. After exclusion of 24 non-Swedish individuals, genotypes were available for 424 unrelated patients and 457 controls from mid Sweden, and from 154 unrelated patients and 194 controls from southern Sweden, resulting in a total of 578 patients and 651 controls available for analysis. The genotypes of the SNP rs10181656 in controls and patients from both cohorts conformed to Hardy–Weinberg equilibrium (p>0.05).
Statistical analysis
Clinical patient characteristics and allele frequencies between groups were compared with χ2 tests. Continuous variables were analysed using Mann–Whitney U test or Kruskal–Wallis test. Fisher's exact test was used to test for Hardy–Weinberg equilibrium of genotypes. OR and 95% CI were calculated from 2 × 2 contingency tables and Mantel–Haenszel estimates were used for summary measures. Univariate and multivariable-adjusted logistic regression analyses estimated the impact of risk factors on ICVD and IHD events. Gender, cohort, 1 or 2 vs 0 STAT4 risk factors and all covariates with p≤0.05 were entered into all inclusive multivariable-adjusted models. Data processing was performed using JMP software (SAS Institute, Carey, North Carolina, USA). For power analysis see supplementary material.
Results
Patients
Characteristics of the patients with SLE are given in table 1. Among the patients, 61 individuals had experienced an ICVD event, of which 10 experienced at least 1 TIA but no stroke. A total of 66 patients had a history of IHD; 15 presented with isolated symptoms of angina pectoris while the remainder had been diagnosed as having MI.
Patient characteristics
Associations between STAT4 risk allele and vascular events
We observed a higher frequency of the STAT4 SNP rs10181656(G) in patients with SLE with previous arterial events, than in patients with SLE without arterial events. There was no association between the STAT4 risk allele and VTE. The association with previous arterial events was mainly attributable to the group of patients with ICVD manifestations, while manifestations of IHD or peripheral ischaemic vascular disease (PIVD) were not associated with the risk allele. When excluding the 10 patients with TIA the association remained of similar magnitude. Results were consistent in the two patient groups and, when combined, the associations were strengthened. Comparison of the risk allele frequency between patients and controls demonstrated that patients with arterial events contributed substantially more to the association signal with SLE as compared to patients free of arterial events (table 2).
Associations of the risk allele, STAT4 single nucleotide polymorphism (SNP) rs10181656 (G), in patients with systemic lupus erythematosus (SLE) with and without previous vascular events (VE)
A dose-dependent relationship between previous manifestations of ICVD and the number of risk alleles was apparent (figure 1). The combined OR for ICVD in patients with SLE homozygous for the rs10181656(G) allele in comparison with other patients with SLE was 3.2 (95% CI 1.7 to 6.2, p=0.0002). In all, 77% of patients with SLE with previous ICVD were carriers of one or two copies of the risk allele.

Percentage of patients with previous ischaemic cerebrovascular disease (ICVD), defined as stroke or transitory ischaemic attack, in relation to STAT4 rs10181656 genotype.
Associations between the STAT4 risk allele and anti-phospholipid antibodies
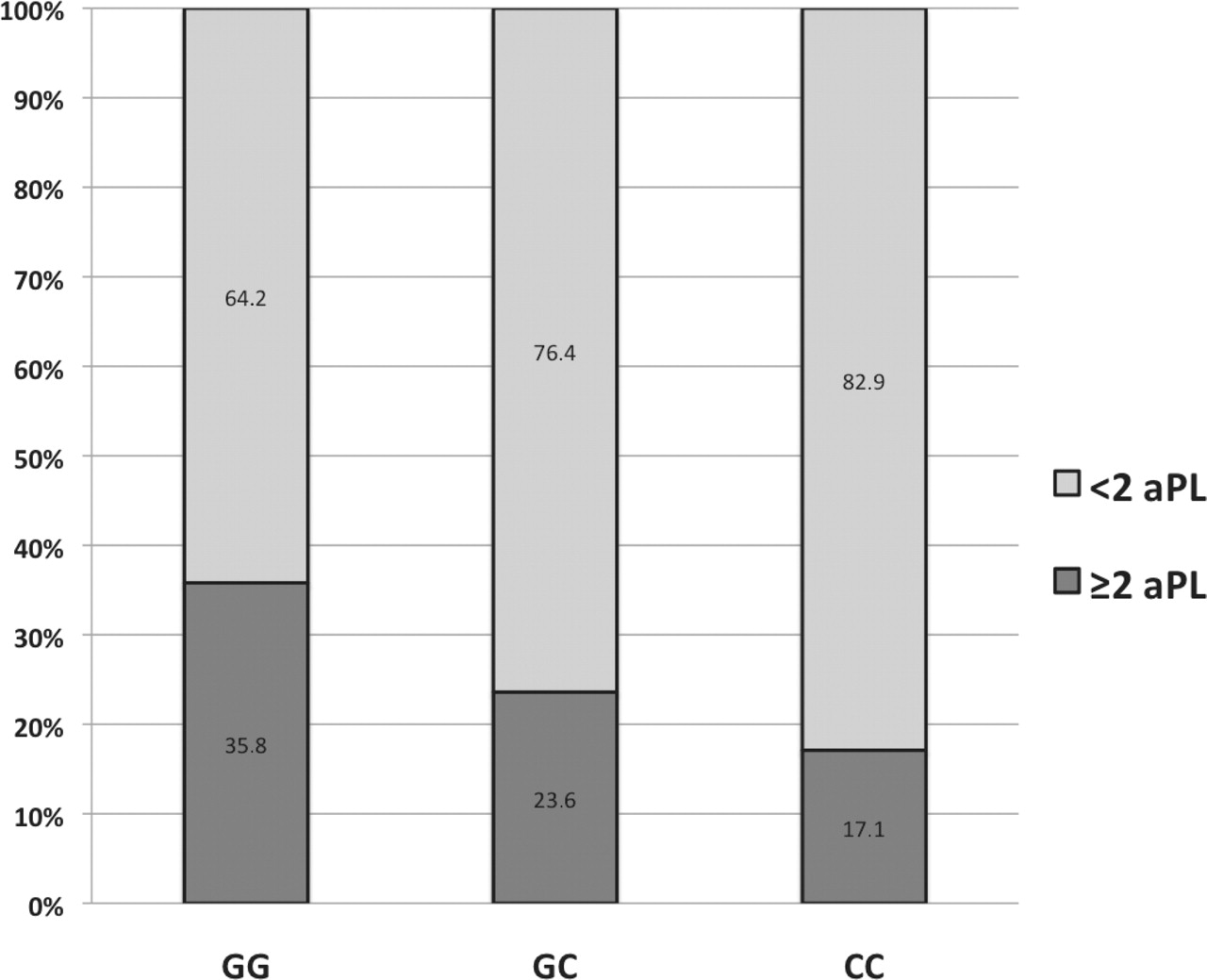
In the mid Sweden cohort STAT4 was associated with the simultaneous occurrence of two or more positive aPL (≥2 aPL) and with a positive LAC test. In the southern Sweden cohort a weak association with a positive test for aCL, IgM and aPT was detected. Analysis of the combined patient groups yielded significant ORs for an association between the STAT4 risk allele and occurrence of ≥2 aPL and a suggestive but non-significant association was observed for aCL IgM and aPT (table 3). There was a dose-dependent relationship in the combined patient groups between the number of STAT4 risk alleles and the percentage of patients with ≥2 aPL (figure 2). The number of risk alleles was also associated with the level of LAC positivity (p=0.002), but not with the level of the individual aPLs (data not shown).
Association of the risk allele, STAT4 single nucleotide polymorphism (SNP) rs10181656 (G) in patients with systemic lupus erythematosus (SLE) with and without positive tests for anti-phospholipid antibodies (aPL)
{kind=link}
{kind=link}
Percentage of patients with a positive test for at least two of the four investigated anti-phospholipid antibody (aPL) specificities (anti-cardiolipin IgG or IgM, anti-β2 glycoprotein 1 or antiprothrombin)=≥2+aPL in relation to STAT4 rs10181656 genotype.
Risk factors for vascular events
Adjustment for available known risk factors did not attenuate the association between the STAT4 risk allele and vascular events. Any STAT4 risk alleles emerged as a strong risk factor for ICVD in patients with SLE (OR=3.3, 95% CI 1.7 to 6.7).
A positive test for aCL IgG also remained as an independent risk factor for ICVD (OR=2.6, 95% CI 1.3 to 4.9). STAT4 genotype did not significantly contribute to the occurrence of IHD or VTE. aPL was associated with ICVD and VTE but there was no convincing association between aPL and IHD (table 4).
Previous ICVD, IHD and VTE in relation to the presence of selected cardiovascular risk factors: logistic regression models
Discussion
Our major finding is that the number of STAT4 risk alleles (SNP rs10181656(G)) is associated with an increased risk of ICVD in SLE in a dose-dependent manner. The risk allele was furthermore associated with occurrence of prothrombotic aPL indicating a possible mechanistic connection between genotype and ICVD phenotype. Our observations imply that STAT4 genotype is a previously unknown major risk factor for ICVD, a feared complication, which affected 10% of the patients in the present study.
The STAT4 risk variants were linked to occurrence of antibodies against double-stranded DNA in previous studies17 21 and we noted an association with the immunological ACR criteria22 (p=0.02, supplementary table 1) and more severe disease, as measured by SLICC/ACR damage index (p=0.03).23 Prothrombotic aPLs are autoantibodies, which target membrane phospholipids and associated protein cofactors. APLs are established risk factors for venous and arterial events.26 They occur in anti-phospholipid syndrome (APS) and are detectable in 25% to 40% of patients with SLE.27 Familial aggregation of APS has been reported and genetic analyses suggest a dominant pattern of inheritance, but the genes involved have not yet been identified.28 We investigated 4 aPL specificities and performed a LAC test on 289 patients from Karolinska University Hospital. LAC is the most relevant test for aPLs associated with thromboembolic manifestations regardless of site and type of thrombosis.26 29 To have antibodies to more than one aPL specificity confers a higher risk of thromboembolic complications as well.26 A clear association between the STAT4 risk allele and the occurrence of two or more aPLs, a positive LAC and a higher level of LAC was present. These observations indicate that the STAT4 risk variant promotes the production of clinically significant aPLs. Two recent studies corroborate our findings demonstrating an association between the STAT4 risk allele and APS.30 31 Our results are also in line with the prominent role of STAT4 in B cell activation and autoantibody production observed in lupus prone mice.32 33 Thus, one mechanism by which STAT4 could increase the risk for ICVD is by an increased production of several prothrombotic aPL.
ICVD and IHD were comparably frequent in our study, however only ICVD was associated with the STAT4 risk allele. ICVD is often a thomboembolic complication while IHD is believed to principally be a consequence of premature atherosclerosis.34 This study demonstrates that traditional risk factors such as smoking, diabetes and gender have a stronger association with IHD than with ICVD in SLE. Additional risk factors such as hyperlipidaemia and markers of systemic inflammation, not investigated in the present study, clearly also contribute to IHD and ICVD.5,–,7 35 36 Apart from this, this study demonstrates that risk profiles for IHD and ICVD may differ, with respect to risk factors other than STAT4 genotype, suggesting differences in the etiopathogenesis of these two types of arterial manifestations in SLE.
The STAT4 risk allele was not associated with VTE despite the association between VTE and aPLs. Many established risk factors for VTE are hereditary and differ from those of arterial thrombosis.37 In longitudinal studies, recurring thrombosis in patients with APS are often of the same type, that is, arterial or venous, as the initial presentation.38 Emerging data also suggest that vessel-specific inflammation39 may be pivotal for development of arterial, but not venous thrombosis.37 Another study demonstrated that serum levels of endothelium-derived endothelin-1, a marker of endothelial activation, were able to discriminate patients with APS with stroke from patients with APS with venous thrombosis.40 Thus, several factors, possibly including STAT4 genotype, may contribute to a personal predisposition for either arterial or venous manifestations in patients with aPL.
STAT4 mediates IL12-dependent activation of natural killer cells and polarisation of naïve CD4 T cells to IFNγ producing T helper (Th)1 cells.18 Th1 cells and IFNγ, which activates macrophages, are prevalent in human carotid arteries and preferentially tend to localise in the rupture prone shoulder regions of atherosclerotic plaques.34 IFNα producing PDCs are also present in atherosclerotic plaques from carotid lesions where they can act as inflammatory amplifiers.41 Recently, it was shown that a STAT4 risk allele, perfectly linked to rs10181656, confers augmented sensitivity to IFNα in patients with SLE.42 Consequently, STAT4 activity could promote the risk of plaque rupture and thrombosis by increasing the local inflammatory response.
Though consecutively gathered these patients with SLE are not random samples. Differences in collection procedures may, as previously described,1 43 44 explain the observed discrepancies between the two SLE groups in this study. The mid Sweden group was collected at University hospitals, which are tertiary academic centres where patients were younger at disease onset and at follow-up. They also had a higher risk allele frequency. The southern Sweden group was collected in Lund where a longitudinal SLE cohort has been well established since the mid 1980s. This epidemiological cohort aims to investigate all cases of lupus in a defined catchment area (Lund–Orup). However, for the present study, consecutively included patients with SLE outside the catchment area were also enrolled. We find our results biologically plausible and, regarding ICVD, they were replicated in two patient groups. Nevertheless, they should be interpreted with some caution since we did not correct for multiple testing. Despite this and differences in collection procedures, the associations between the STAT4 risk allele and ICVD were replicated and of similar magnitude and direction in both SLE groups, supporting the robustness of our results. Further studies are clearly needed to understand why STAT4 risk alleles are associated with ICVD, but not with other types vascular events.
In conclusion our data demonstrate that the STAT4 genotype is associated with SLE-related ICVD and with prothrombotic aPLs, but not with IHD or VTE. ICVD is an important manifestation of CVD, a major cause of premature mortality among patients with SLE. Here, we can for the first time identify a genetic contribution, which seems to predispose some patients with SLE to ICVD. Whether STAT4 genotype also contributes to clinical presentation with ICVD in primary APS, other chronic inflammatory conditions, or in the general population remains to be determined. However, STAT4 risk alleles have recently been associated with other autoimmune diseases among them rheumatoid arthritis, type 1 diabetes and inflammatory bowel disease,16 45,–,47 all of which are associated with cardiovascular comorbidities.
Acknowledgments
We thank Anna-Britta Johansson for analysing aPL results, Eva Jemseby for handling of blood samples, Chuan Wang for technical assistance with genotyping, and Ingrid Kockum and Elisbeth Berg for statistical advice.
References
Supplementary materials
Web Only Data ard.2009.115535
Files in this Data Supplement:
Footnotes
JG, DL and JS contributed equally to this work.
-
Funding Funding was received from the Alliance for Lupus Research, the Swedish Research Council, the Swedish Rheumatism Foundation, the Uppsala University Hospital Research and Development Fund, Ulla and Roland Gustafssons Foundation, the Swedish Heart-Lung Foundation, The King Gustaf V 80th Birthday Fund, The Swedish Society of Medicine, The Åke Wiberg Foundation, Alex and Eva Wallstöms Foundation, Karolinska Institutet Foundations, the Knut and Alice Wallenberg Foundation, ALF funding from Stockholm County Council and COMBINE.
-
Competing interests None.
-
Ethics approval This study was conducted with the approval of the Local ethics committees at Karolinska University Hospital, Uppsala University Hospital and Lund University hospital.
-
Provenance and peer review Not commissioned; externally peer reviewed.