Article Text

Abstract
Objectives Classification criteria are biased towards classifying long-standing disease. We compared the European League Against Rheumatism (EULAR)/American College of Rheumatology (ACR)-2019, Systemic Lupus International Collaborating Clinics (SLICC)-2012 and ACR-1997 criteria in an early (median 48 months) systemic lupus erythematosus (SLE) cohort.
Methods Patients diagnosed with SLE (n=690) or control diseases (n=401). Sensitivity, specificity of the criteria and time-to-classification were calculated. Modified classification algorithms were derived from a random 80% and validated in the remaining 20% of the dataset running multiple iterations.
Results At last assessment, sensitivities of ACR-1997, SLICC-2012 and EULAR/ACR-2019 criteria were 85.7%, 91.3% and 88.6%, with specificities 93.0%, 93.8% and 97.3%, respectively. Both SLICC and EULAR/ACR enabled earlier classification. Only 76.7% of patients with SLE met all three criteria suggesting non-overlapping groups. Notably, unclassified patients had high prevalence of British Isles Lupus Assessment Group moderate/severe manifestations (43.3%–60%) and SLICC/ACR organ damage (30%–50%). At diagnosis, criteria missed 25.6%–30.5% of patients. Modification of EULAR/ACR and SLICC algorithms to include hypocomplementaemia and/or positive anti-phospholipid antibodies as alternative entry criterion, and/or allow classification with fewer clinical criteria from multiple organs, increased their sensitivity at diagnosis (median 82.0% and 86.2%) and overall (93.7% and 97.1%) with modest decreases in specificity. Importantly, patients who were still missed by the modified criteria had lower incidence of major organ involvement, use of immunosuppressive/biological therapies and organ damage.
Conclusions The SLICC and EULAR/ACR are more sensitive than the ACR and the EULAR/ACR criteria have superior specificity in early SLE, although patients with significant disease can be missed. Combination and/or modification of the classification algorithms may enhance their sensitivity, allowing earlier classification and treatment of more patients with high disease burden.
- systemic lupus erythematosus
- autoimmune diseases
- outcomes research
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Systemic lupus erythematosus (SLE) classification criteria have been developed to classify homogeneous patient groups in epidemiological studies and clinical trials but they are often used to aid disease diagnosis.
What does this study add?
Both the European League Against Rheumatism (EULAR)/American College of Rheumatology (ACR) and the Systemic Lupus International Collaborating Clinics (SLICC) criteria have increased sensitivity with superior specificity of the EULAR/ACR criteria in early SLE and enable earlier classification as compared with the ACR criteria.
All three sets of criteria may miss or delay the classification of a proportion of patients with SLE with moderate/severe disease, particularly cases of neurological-dominant lupus.
The criteria may classify non-overlapping groups of patients with SLE; their combination ensures maximum patients capture in clinical studies.
Modification of the EULAR/ACR and SLICC criteria by lowering the classification thresholds may enhance their sensitivity both at early disease stages and later.
How might this impact on clinical practice or future developments?
Use of all three existing sets of criteria may ensure maximum capture of more representative groups of patients with SLE for clinical studies.
Pending validation in prospective studies, modification of the SLE classification algorithms may improve their performance especially in early disease.
Introduction
Classification criteria for systemic lupus erythematosus (SLE) have been developed to ensure the inclusion of homogeneous groups of patients in clinical studies.1 Nonetheless, these criteria are often used in clinical practice to aid diagnosis. In this regard, the Systemic Lupus International Collaborating Clinics (SLICC) 2012 criteria2 were reported to have increased sensitivity3–5 and capture more patients at the population level,6 7 as compared with the American College of Rheumatology (ACR) 1997 criteria.8 Still, clinical diagnosis may precede classification,9 10 suggesting that especially at early stages, not all individuals with SLE will fulfil the criteria. Moreover, organ-dominant forms may occur imposing further classification challenges.
Recently, the European League Against Rheumatism (EULAR) jointly with the ACR have introduced new classification criteria,11 12 which are based on two novel concepts, namely antinuclear antibodies(ANA) as an entry criterion coupled with variably weighed features.13 Whether the new criteria have higher accuracy and allow for earlier classification merits investigation across different cohorts. The prognostic implications of classifying or not patients with SLE with the existing criteria is also not known.
We compared the three classification criteria in a large cohort of patients with early diagnosis of SLE or other rheumatological diseases, spanning from the community to tertiary care. Sensitivity was determined at the time of diagnosis and also, at last follow-up; we also examined which criteria enabled earlier classification. Guided by our observation that criteria classify non-overlapping patient groups, we compared the phenotypic characteristics and outcomes among patients who are unclassified by each criterion. Based on our sample characteristics, we propose modifications in the classification algorithms to assure the highest combination of sensitivity and specificity, thus allowing earlier classification and treatment of patients with potentially high disease burden.
Methods
Setting and participants
We performed a retrospective observational study in two centres. The Department of Rheumatology, University Hospital of Heraklion, serves as referral centre for autoimmune diseases on the island of Crete (population 0.6M), connects to a cooperative network of private rheumatologists and general physicians, and provides inpatient and outpatient services from primary to tertiary level.9 The Rheumatology Clinic, Attikon University Hospital, covers 1.7 M citizens in Western Attica.14 Both centres have established SLE registries and use homogenised, structured forms for collecting detailed demographics, clinical characteristics (including classification criteria), use of treatments and disease outcomes.9 We included consecutively registered cases diagnosed during 01/2005-12/2016 with SLE or other rheumatological diseases by consultant rheumatologists with ≥5 years clinical practice (online supplementary methods, online supplementary figure S1). We selected this diagnosis time interval to ensure data completeness and reduce possible information/classification bias. Additional inclusion criteria were as follows: sufficient patient identification and clinical data, age of diagnosis ≥16 years, known ANA status and follow-up ≥6 months to confirm the diagnosis. The study was approved by the local Ethics Committees.
Supplemental material
Supplemental material
Data collection, criteria and attribution
For each patient, demographics, rheumatological disease and date of diagnosis, presence and date of earliest reported occurrence of the items from all three classification criteria sets,2 8 11 12 and date of last follow-up visit/assessment were extracted from medical charts. Neuropsychiatric manifestations were assessed through multidisciplinary approach15 and ascertained by the use of the Italian Study Group attribution model16 (online supplementary methods). Attribution of the criteria items to SLE or not was arbitrated by rheumatologists (DB, GB and AF) with special interest and experience in the disease, and according to the EULAR/ACR attribution process11 12 The date of appearance of each item was considered either the date of the visit that this was first documented. A few patients with no documentation of immunological tests were considered negative for these items. Patients with unknown ANA were excluded (online supplementary figure S1).
Disease outcomes
Presence and corresponding date of each item of the SLICC/ACR damage index17 was monitored. Severity of disease manifestations was classified with the British Isles Lupus Assessment Group (BILAG) system.18 Use of immunosuppressive/biological treatments and physician global assessment of SLE severity were collected9 19 (online supplementary methods)
Statistical analysis
Sensitivity of the criteria was assessed against physician diagnosis, both at the time of diagnosis (extended by 3 months to allow completion of diagnostic work-up) and at last patient visit/assessment (overall sensitivity). Patients with unverified date of appearance of any criteria item were included only in the overall sensitivity analysis. Specificity was determined against patients with other rheumatological diseases. We produced a likelihood ratios graph of the three sets of criteria.20 In separate analysis, we calculated the earliest date of fulfilment of each set of criteria and the time elapsed since the date of the earliest item. Hazard analysis was used to determine the median (95% CI) time-to-classification for each set of criteria. Between-groups comparisons were performed by the McNemar’s test or linear mixed model analysis for partially paired samples. All analyses were performed using SPSS V.24.0.
Results
The EULAR/ACR and SLICC criteria have increased sensitivity and enable earlier classification
We assessed the performance of the three classification criteria in patients diagnosed with SLE (n=690) or other rheumatological diseases (n=401) (online supplementary table S1). Both the EULAR/ACR and SLICC had higher sensitivity (88.6% and 91.3%, respectively) than the ACR criteria (85.7%), with the EULAR/ACR having higher specificity than the other two sets (97.3% vs 93.0%–93.8%) (figure 1A). Accordingly, the EULAR/ACR criteria had lower false-positive rate, whereas the SLICC had higher true-positive rate (figure 1B). Only 2.9% of SLE cases were missed by all three criteria, suggesting that their combination enables the classification of the vast majority of patients encountered in clinical practice.
Supplemental material

The EULAR/ACR 2019 and SLICC 2012 criteria have increased sensitivity and allow earlier classification in patients with SLE as compared with the ACR 1997 criteria. (A) Sensitivity and specificity (assessed at the time of last patient assessment/visit) of the EULAR/ACR 2019, SLICC 2012 and ACR 1997 criteria as well as their combination, both in the total of patients with SLE (n=690) and disease controls (n=401) and within the respective ANA-positive subgroups (n=646 and n=159, respectively). (B) Modified plot of true-positive rate and false-positive rate20 for the EULAR/ACR 2019, SLICC 2012 and ACR 1997 criteria. The blue shaded region corresponds to superior performance of the EULAR/ACR 2019 over SLICC 2012 criteria in confirming the absence of SLE (ie, increased specificity). the yellow shaded region corresponds to superior performance of the SLICC 2012 over EULAR/ACR 2019 criteria in confirming the presence of SLE (ie, increased sensitivity). The lower-right position of the ACR 1997 plot corresponds to its inferior classification performance as compared with the SLICC 2012 and EULAR/ACR 2019 criteria. (C) Sensitivity of the three classification criteria within the subgroup of patients with SLE with early disease (duration <3 years). (D) Time-to-classification (time elapsing between the date of first appearance of the earliest criteria (belonging to any of the three sets) until the earliest date of fulfilment of each set of criteria) analysis for each set of classification criteria within the subgroup of patients with SLE with early disease (as in B). *p<0.05; **p<0.01; ***p<0.001. ACR, American College of Rheumatology; EULAR, European League Against Rheumatism; SLE, systemic lupus erythematosus; SLICC, Systemic Lupus International Collaborating Clinics.
By analysing patients with disease duration <3 years, we found significantly increased sensitivity of the EULAR/ACR (87.3%) and SLICC (91.4%) as compared with the ACR criteria (79.9%, p<0.01 and p<0.001, respectively) (figure 1C). In this group, the median (95% CI) time interval between the earliest item and fulfilment of the criteria was shorter for the EULAR/ACR (9.1 (6.5–11.8) months) and SLICC (9.1 (6.9–11.3) months) than the ACR (12.1 (9.6–14.7) months, p=0.043 and p=0.001, respectively) criteria (figure 1D). Together, both the EULAR/ACR and SLICC criteria have increased sensitivity in early SLE and enable earlier classification than the ACR criteria.
Existing criteria may miss or delay classification in a proportion of patients especially with neurological SLE
Patients with SLE with major organ disease often require immunosuppressive therapy and accrue more damage. All three criteria had lower sensitivity for classifying neurological versus renal SLE (81.7%–91.7% vs 93.0%–96.5%, respectively) (figure 2A, online supplementary table S2). The SLICC criteria had increased sensitivity for haematological manifestations. Depending on the criteria set, 7.1%–17.3% of patients with moderately severe or severe disease (BILAG) were not classified. Notably, the combination of all three criteria ensured the maximum capture of major disease subgroups (93.7%–98.5%) (figure 2A).
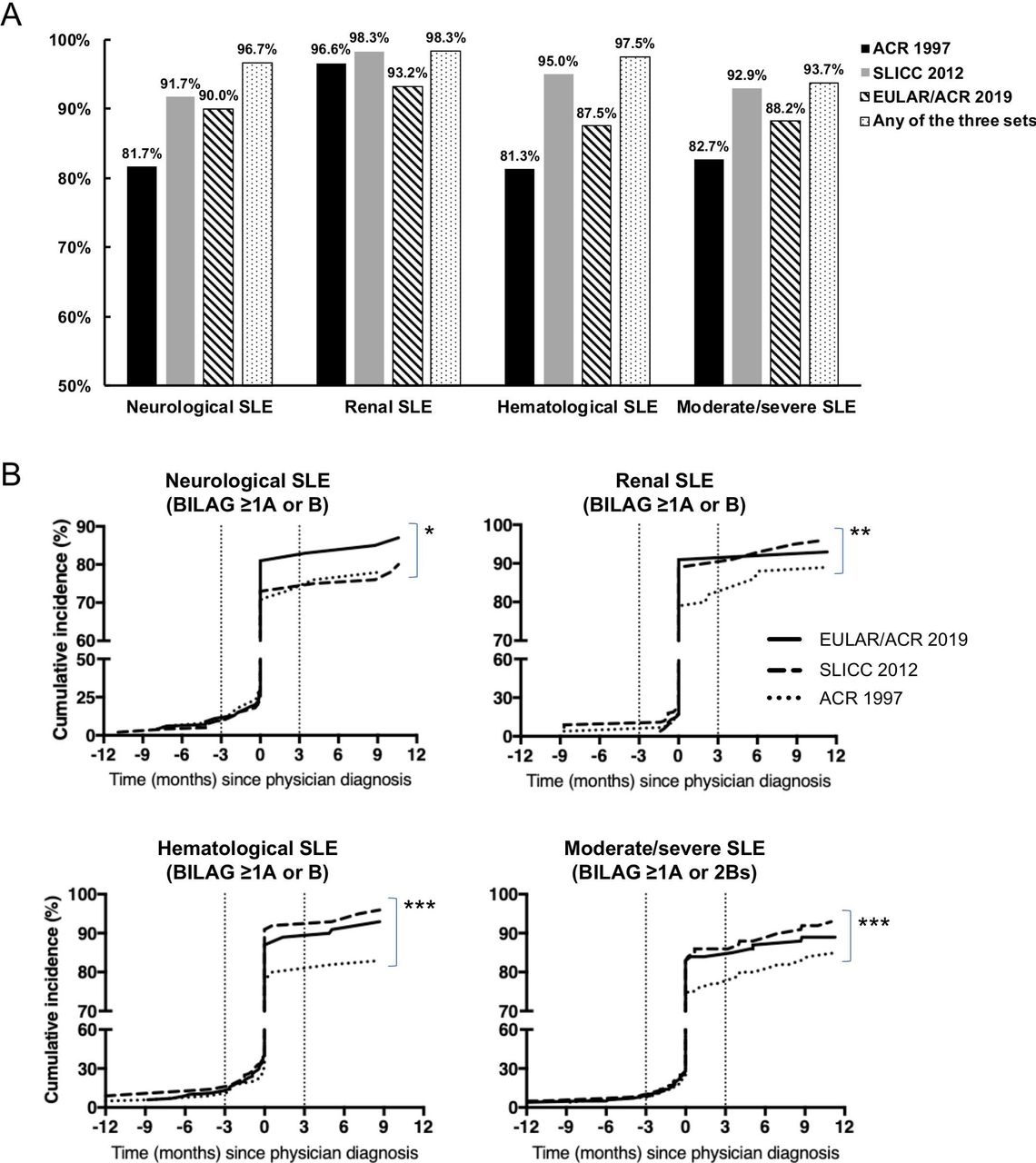
Existing criteria may miss or delay the classification of patients with SLE with major organ disease especially neurological SLE. (A) Sensitivity of the EULAR/ACR 2019, SLICC 2012 and ACR 1997 criteria as well as their combination across subgroups of patients with SLE with major organ disease. Neurological, renal and haematological disease were defined as history of activity from the respective organs/domains classified as BILAG B or A. Moderate/severe SLE was defined as history of at least 1 BILAG A or 2 BILAG Bs active manifestations (from any organ/domain). (B) Timing of SLE classification (according to the EULAR/ACR 2019, SLICC 2012, ACR 1997 criteria) in reference to physician diagnosis within the subgroups of patients with SLE with neurological, renal, haematological and overall moderate/severe disease (defined as above). The x-axis represents the difference (in months) in the time of criteria classification compared with diagnosis. *p<0.05 for the comparison of the EULAR/ACR 2019 versus ACR 1997 criteria (Wilcoxon signed-rank test); **p<0.01 for the comparison of the EULAR/ACR 2019 versus ACR 1997 and the SLICC 2012 versus ACR 1997 criteria (Wilcoxon signed-rank test); ***p<0.001 for the comparison of the EULAR/ACR 2019 versus ACR 1997 and the SLICC 2012 versus ACR 1997 criteria (Wilcoxon signed-rank test). ACR, American College of Rheumatology; BILAG, British Isles Lupus Assessment Group; EULAR, European League Against Rheumatism; SLE, systemic lupus erythematosus; SLICC, Systemic Lupus International Collaborating Clinics.
We also compared the timing of classification against physician diagnosis within classified patients with SLE. Although classification concurred with or antedated diagnosis in the majority of cases, still, diagnosis predated classification by >3 months in 17.3%–19.9% (online supplementary table S3). In agreement with sensitivity, increased rates of delay between classification and diagnosis were noted for neurological (20.0%–26.8%) versus renal (7.7%–14.8%) SLE (online supplementary table S3, figure 2B). Across all patient subgroups with major disease, the SLICC and EULAR/ACR enabled earlier classification than the ACR criteria (figure 2B).
The three sets of criteria classify non-overlapping groups of patients with SLE
Only 76.7% of patients with SLE met all three classification criteria, suggesting non-overlapping patient groups. To decipher the ability of criteria to classify distinct disease phenotypes, we compared patients who were missed by each one of the criteria sets and by all three of them (table 1). Patients who did not meet the ACR criteria had significantly higher prevalence of haematological and immunological features. Patients who were unclassified by the EULAR/ACR had increased rates of mucocutaneous disease and leucopaenia, whereas those missed by the SLICC criteria had predominant skin and joints disease. Among patients who were not classified by any of the criteria, 20% had neurological manifestations, whereas the prevalence of immunological features was lower. Together, existing criteria capture non-identical groups of patients with SLE.
Prevalence of clinical and immunological features (SLICC 2012 criteria) across groups of patients with SLE who were not classified by the classification criteria
Patients with SLE missed by the classification criteria may exhibit high disease burden
Next, we asked whether patients who are missed by the criteria differ in terms of disease outcomes. To this end, we assessed the severity of lupus manifestations and irreversible organ damage across the aforementioned groups of patients. Irrespective of the criteria used, a significant proportion (43.3%–55.7%) of non-classified patients had moderate/severe manifestations which required immunosuppressive or biological treatment (figure 3A). Concordantly, organ damage developed in 30.0%–40.5% of unclassified patients (figure 3B). Notably, patients missed by all three criteria also exhibited significant disease burden (45.0% severe manifestations, 50.0% with organ damage). These results suggest that despite their high sensitivity, classification criteria may miss patients with potentially severe disease.
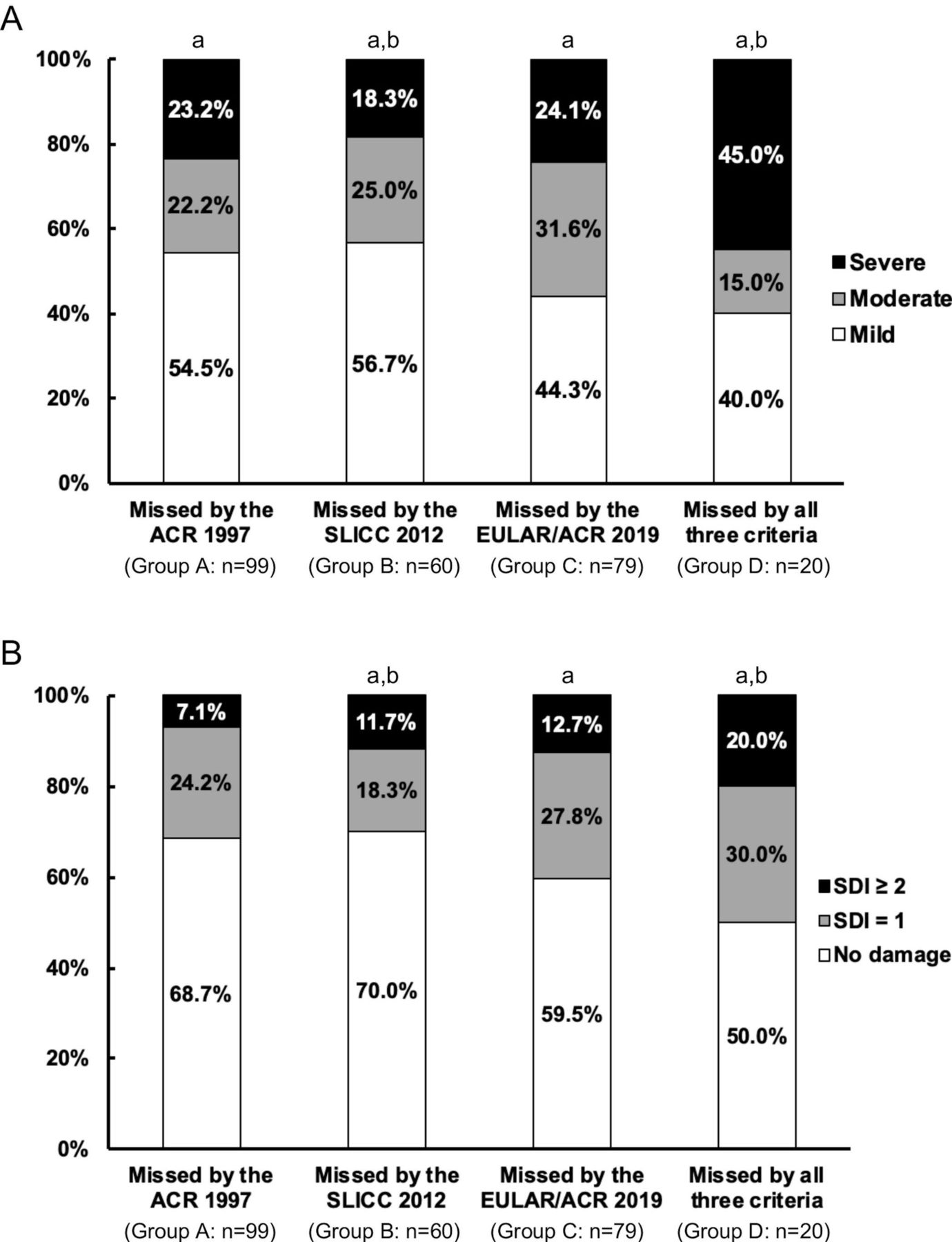
Patients with SLE who are missed by the classification criteria exhibit a high disease burden with high rates of moderate/severe disease and organ damage. (A) Distribution of disease severity (physician global assessment: mild, moderate, severe) across groups of patients with SLE who are not classified by the ACR 1997 (Group A), SLICC 20012 (Group B), EULAR/ACR 2019 (Group C) and all three classification criteria (Group D). Between-group comparisons were performed with linear mixed models to account for partially paired data. a Statistically significant difference in prevalence of severe manifestations between group D and groups A, B, C (p<0.05: group D vs groups A, C; p=0.001: group D vs group B); b p=0.037 for the difference in disease severity (moderate/severe manifestations) between group B and group D. (B) Organ damage accrual based on the SDI (assessed at last patient visit/assessment) across the aforementioned patient groups. a,b statistically significant difference in prevalence of organ damage (SDI>0) between group B and groups C (p=0.008) and group D (p=0.015). ACR, American College of Rheumatology; EULAR, European League Against Rheumatism; SDI, SLICC damage index; SLE, systemic lupus erythematosus; SLICC, Systemic Lupus International Collaborating Clinics.
Modified classification algorithms show enhanced accuracy for SLE classification
In view of the above, we explored alternative classification algorithms based on the existing criteria to enhance their accuracy. We focused on the EULAR/ACR and SLICC criteria as they displayed the highest sensitivity, and extracted a random 80% (derivation) set of our total sample (SLE and controls) to identify subgroups of patients who failed classification and assess the frequency of individual items over the entire observation period (online supplementary figure S2). Patients unclassified by the EULAR/ACR criteria included primarily cases who (a) did not meet the entry criterion of positive ANA, yet they had hypocomplementemia and/or positive anti-phospholipid antibodies and (b) met the entry criterion, scored ≥6 from the clinical domains/criteria but their aggregate clinical and immunology score was eight or 9, thus falling short of the classification threshold.13 In the case of the SLICC criteria, two major groups of non-classified patients included those with (a) single immunological criterion and two clinical criteria from different organs/domains and (b) no immunological criteria but ≥4 clinical criteria from ≥2 different organs/domains. Most of the patients in these two groups had ACR-defined photosensitivity, which was included as additional clinical criterion to preserve the sensitivity/specificity ratio.
Supplemental material
By amending the classification algorithms to include the aforementioned patient groups, the sensitivity of the ‘modified’ EULAR/ACR and SLICC criteria in the derivation set increased by 5.5 and 6.1 percent units, respectively, with modest decreases in specificity (online supplementary table S6). We tested the modified algorithms in the remaining 20% of the sample running 100 iterations to account for patient heterogeneity. The median sensitivity of the modified EULAR/ACR and SLICC criteria in the validation sets were 93.7% and 97.1%, respectively, with corresponding specificities 94.9% and 90.2% (figure 4A, online supplementary table S6).

Modified classification algorithms based on the SLICC 2012 and EULAR/ACR 2019 criteria have increased sensitivity and accuracy for classifying SLE. (A) Box-plot of the sensitivity (upper panel), specificity (middle panel) and accuracy (lower panel) of the original and modified versions of the classification criteria assessed over the entire observation period. results are derived from 100 random iterations in the validation datasets (20% of total sample of patients with SLE and disease controls). Horizontal lines represent median values. See the Methods section for more details. modified SLICC 2012 classification: (a) ≥5 clinical criteria (including the SLICC 2012 clinical criteria and ACR 1997-defined photosensitivity) and NO immunological criterion; (b) ≥3 clinical criteria (including the SLICC 2012 clinical criteria and ACR 1997-defined photosensitivity) and ≥1 immunological criterion; modified EULAR/ACR 2019 classification: (a) ANA test is negative but there is hypocomplementaemia (low C3 and/or) C4 and/or positive anti-phospholipid antibodies (alternative entry criterion) and EULAR/ACR 2019 clinical score is ≥10; (b) ANA-positive, negative for other immunological tests (EULAR/ACR 2019 immunological score=0), EULAR/ACR 2019 clinical score is ≥8 and ACR 1997-defined photosensitivity is present; (c) ANA-positive, EULAR/ACR 2019 immunological score is ≥2 and EULAR/ACR 2019 clinical score is ≥6. (B) Box-plot of the sensitivity (upper panel), specificity (middle panel) and accuracy (lower panel) of the original and modified versions of the classification criteria assessed at the time of physician diagnosis (extended by 3 months) (100 iterations, validation sets). ACR, American College of Rheumatology; EULAR, European League Against Rheumatism; SLE, systemic lupus erythematosus; SLICC, Systemic Lupus International Collaborating Clinics.
At the time of physician diagnosis (extended by 3 months for completion of work-up, ‘t0’), the sensitivity of the criteria ranged 69.5%–75.4% (online supplementary table S7). By applying the same modified EULAR/ACR and SLICC classification algorithms at ‘t0’, we confirmed increases in sensitivity by 7.3% and 12.2%, with reductions in specificity by 1.3% and 2.5%, respectively (figure 4B, online supplementary table S7). Collectively, modifications of the classification algorithms may enhance their accuracy although vigilance will be needed to avoid misclassification of patients with non-lupus.
The modified criteria classify more patients with SLE with early disease progression
Our results demonstrated high disease burden among patients who were missed by the classification criteria (figure 3). We therefore asked whether the modified classification algorithms had increased sensitivity over the original versions in capturing severe forms of the disease. Initially, we focused on early disease stages and grouped patients according to whether they fulfilled or not the original and modified versions of SLICC and EULAR/ACR criteria at t0. These groups were then monitored for new-onset adverse outcomes (BILAG A/B activity from the renal, neurological or haematological domains, use of immunosuppressive or biological treatments, organ damage) during the first 6–24 months since diagnosis. We observed a high incidence of adverse disease outcomes in patients missed by the original criteria at t0, although lower compared with classified patients (figure 5). Rates of all three outcomes were significantly lower (by 17% to 44%, p≤0.017) among patients who were missed by the modified than the original EULAR/ACR and SLICC criteria. Similarly, the modified criteria captured significantly more patients with moderate/severe SLE and organ damage as compared with the original versions (online supplementary figure S3A,B). Accordingly, modified algorithms show increased sensitivity for classifying severe/progressive forms of SLE and likewise, patients who are unclassified by the modified criteria manifest milder disease.
Supplemental material

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Patients with SLE missed by the modified versions of the SLICC 2012 and EULAR/ACR 2019 classification criteria demonstrate significantly lower incidence of adverse disease outcomes at early stages. (A) Incidence of BILAG B or BILAG A activity from the neurological, renal and/or haematological domains in patients with SLE who—at the time of physician diagnosis—are as follows: (i) classified (circle) or not (square) by the original EULAR/ACR 2019 (or SLICC 2012) criteria, (ii) are missed by the modified version of the EULAR/ACR 2019 (or SLICC 2012) criteria (triangle) and (iii) are missed by both the modified version of the EULAR/ACR 2019 (or SLICC 2012) criteria and the remaining two criteria (original versions) (diamond). modified SLICC 2012 classification: (a) ≥5 clinical criteria (including the SLICC 2012 clinical criteria and ACR 1997-defined photosensitivity) and NO immunological criterion; (b) ≥3 clinical criteria (including the SLICC 2012 clinical criteria and ACR 1997-defined photosensitivity) and ≥1 immunological criterion; modified EULAR/ACR 2019 classification: (a) ANA test is negative but there is hypocomplementemia (low C3 and/or) C4 and/or positive anti-phospholipid antibodies (alternative entry criterion) and EULAR/ACR 2019 clinical score is ≥10; (b) ANA-positive, negative for other immunological tests (EULAR/ACR 2019 immunological score=0), EULAR/ACR 2019 clinical score is ≥8 and ACR 1997-defined photosensitivity is present; (c) ANA-positive, EULAR/ACR 2019 immunological score is ≥2 and EULAR/ACR 2019 clinical score is ≥6. (B) Incidence of use of high-potency immunosuppressive and/or biological treatments due to active SLE in the same patient groups as in A. (C) Incidence of organ damage accrual (SDI>0) in the same patient groups as in a. statistical comparisons in panels A–C are performed by linear mixed model (repeated measures) analysis for partially matched data across the groups missed by the original criteria, missed by the modified version of the criteria, and missed by the modified version and the other two (original) sets of criteria. ACR, American College of Rheumatology; BILAG, British Isles Lupus Assessment Group; EULAR, European League Against Rheumatism; SDI, SLICC damage index; SLE, systemic lupus erythematosus; SLICC, Systemic Lupus International Collaborating Clinics.
Discussion
We compared the EULAR/ACR and previous classification criteria against clinical SLE diagnosis, focusing also on the prognostic implications of classification. Our results demonstrate that despite improved sensitivity of the EULAR/ACR and SLICC criteria, classification may be missed or delayed in some patients, including patients with high disease burden. Criteria classify non-overlapping patient groups suggesting that their combinatorial use may ensure maximum capture of patients with SLE with diverse presentations. By adjusting the classification thresholds, the sensitivity and accuracy of the criteria for classifying SLE—including severe/progressive forms of the disease—is enhanced.
Classification criteria enable the highest possible inclusion of patients with confirmed disease in clinical studies. Previous reports suggested increased sensitivity of the SLICC—with comparable or lower specificity—than the ACR criteria.4 5 10 21 22 We found greater sensitivity of both SLICC and EULAR/ACR over the ACR criteria, with higher specificity of the EULAR/ACR criteria. The superior performance of SLICC and EULAR/ACR was more evident within patients with early disease, which agrees with published results comparing the SLICC against the ACR criteria.5 This was further corroborated by our time-to-classification analysis showing earlier classification with the EULAR/ACR and SLICC criteria.
Differences between our results with those in other cohorts might be due to various factors such as the ethnic/demographic background of patients, disease duration and inclusion of disease controls. Our study included exclusively Caucasians with average disease duration <5 years, which is lower than other studies.5 Moreover, the frequency of ANA was 93.6%, which is similar to that in a contemporary international SLE cohort (92.3%),23 yet lower than the estimates of a large meta-analysis of epidemiological studies (97.8%, 95% CI: 96.8% to 98.5%).24 This might be explained by our cohort characteristics such as the short disease duration, white/Caucasian ethnicity and older age of onset (median 42 years).23 25 Due to high clinical suspicion, 39 out of 44 ANA-negative patients had been repeatedly tested by standard indirect Hep-2 immunofluorescence (1:80 dilution). Within ANA-positive patients, our sensitivity of the EULAR/ACR criteria was higher (94.6%) and similar to the SLICC criteria (94.7%) (figure 1A), which agrees with the results from the EULAR/ACR validation cohort.11 12
In patients with major organ involvement, early treatment initiation is critical to ensure good outcomes.26–29 Notably, all three criteria had lower sensitivity for neurological than renal SLE. Likewise, the delay between classification and physician diagnosis was greater in neurological disease. It has long been recognised that some patients with lupus may present with organ-dominant/limited disease particularly involving the nervous system, kidneys or blood,1 30 and before sufficient number of criteria accrue to meet classification. In recognition of this, the SLICC first introduced the renal stand-alone criterion for classifying renal-dominant lupus,2 and the EULAR/ACR have introduced higher-weighted items to enable classification with fewer number of afflicted organs.13 To this end, the EULAR/ACR criteria enabled earlier classification of neurological SLE (figure 2B), which represents a step forward this unmet need.
The three sets of criteria vary in the number and diversity of included manifestations, their definition, weighing score and the algorithms to qualify for classification. Only 76.7% of patients with SLE met all three criteria and likewise, the combination of all three criteria enabled maximum capture of patients. By comparing patients who were missed by each of the three criteria, significant differences were noted in prevalence of individual features especially from the mucocutaneous, musculoskeletal, haematological and immunological domains (table 1), suggesting that criteria may classify non-overlapping groups. This might have implications in clinical trial design as it is possible that different manifestations may respond differently to therapeutic agents.31
In agreement with previous reports,10 we noted that at the time of clinical diagnosis, the sensitivity of the criteria was modest. Detailed analysis revealed that physicians often relied on only a few features to secure diagnosis at early stages. This prompted us to devise ‘lower threshold’ EULAR/ACR and SLICC classification algorithms by introducing alternative ‘entry criterion’ in the case that ANA test is negative, and/or allowing the classification of patients with fewer criteria from multiple organs. The new algorithms exhibited enhanced sensitivity with modest decreases in specificity for classifying SLE both at early stage and later during the disease course. Importantly, patients who were missed by the modified criteria exhibited lower rates of adverse outcomes. These findings raise the possibility that modifications of the classification algorithms could be exploited as putative tools in clinical practice. Pending verification, classification criteria can only aid in the diagnosis of SLE and judgement by an experienced SLE specialist is typically required.
Our study is limited by its retrospective design and data extraction from medical records; accordingly, some clinical information may have been missed or underestimated. Nonetheless, both centres maintain detailed patient registries and use structured forms for collecting clinical data, which helps to reduce possible information/data completeness bias. Direct Coombs was not routinely performed before the publication of the SLICC criteria2 (unless in suspected autoimmune haemolysis), which could have underestimated the sensitivity/specificity of SLICC. By analysing patients diagnosed since 2012 (n=354 SLE, n=202 controls), we obtained comparable results with those in the total cohort (SLICC sensitivity: 92.7%, specificity: 93.2%).
In summary, the rheumatologic community has gradually refined the classification criteria taking into consideration caveats in their use. The ACR-1997 criteria acknowledged that ANA positivity was not essential for the classification but some organs/domains were over-represented. The SLICC-2012 introduced the concept of ‘organ-dominant’ disease in the case of nephritis. More recently, the EULAR/ACR-2019 criteria have remedied the over-representation of some organs/domains by introducing the weighting of various manifestations, thus gaining in specificity.
Herein, we have evaluated the performance of the new compared with the previous SLE classification criteria in a large patient cohort. The EULAR/ACR and SLICC criteria have increased sensitivity but classification may be missed or delayed especially at early stages and in cases of neurological lupus. Modification of the classification algorithms may enhance their sensitivity, potentially allowing earlier classification and treatment of patients with potentially severe disease.
Acknowledgments
We are thankful to the staff physicians and nurses of the Rheumatology Departments of the University Hospital of Iraklio and 'Attikon' University Hospital of Athens for providing care to the patients with SLE and other rheumatological diseases.
References
Footnotes
Handling editor Josef S Smolen
Twitter @george_bertsias
Contributors CA, DN and AF collected data from patient medical charts and also performed data entry. I. Genitsaridi performed part of the statistical analyses (time-to-classification, 80/20 validation of the modified criteria). AB organised the RedCap database and assisted in data analyses. EK and EP contributed in the maintenance of the Cretan Lupus Registry and assisted in data collection. I. Gergianaki contributed in the establishment of the Cretan Lupus Registry and the selection of candidate study participants. PS assisted in patient recruitment and reviewed the manuscript. DB and GB conceived and supervised the study. GB performed statistical analyses. CA and GB drafted the manuscript.
Funding The study received funding by the Hellenic Society of Rheumatology & Professionals Union of Rheumatologists of Greece (protocol number: 644), the Pancretan Health Association and the Foundation for Research in Rheumatology (FOREUM; protocol number: 016BertsiasPrecl).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the Ethics Committee of the University Hospital of Iraklio (protocol no. 13960/10-10-2018) and the Ethics Committee of the ‘Attikon’ University Hospital of Athens.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.