Article Text

Abstract
Objectives To compare the efficacy to prevent flares of maintenance versus withdrawal of 5 mg/day prednisone in systemic lupus erythematosus (SLE) patients with clinically quiescent disease.
Methods A monocentric, 12-month, superiority, open-label, randomised (1:1) controlled trial was conducted with 61 patients continuing 5 mg/day prednisone and 63 stopping it. Eligibility criteria were SLE patients who, during the year preceding the inclusion, had a clinically inactive disease and a stable SLE treatment including 5 mg/day prednisone. The primary endpoint was the proportion of patient experiencing a flare defined with the SELENA-SLEDAI flare index (SFI) at 52 weeks. Secondary endpoints included time to flare, flare severity according to SFI and British Isles Lupus Assessment Group (BILAG) index and increase in the Systemic Lupus International Collaborating Clinics (SLICC) damage index (SDI).
Results Proportion of patients experiencing a flare was significantly lower in the maintenance group as compared with the withdrawal group (4 patients vs 17; RR 0.2 (95% CI 0.1 to 0.7), p=0.003). Maintenance of 5 mg prednisone was superior with respect to time to first flare (HR 0.2; 95% CI 0.1 to 0.6, p=0.002), occurrence of mild/moderate flares using the SFI (3 patients vs 12; RR 0.2 (95% CI 0.1 to 0.8), p=0.012) and occurrence of moderate/severe flares using the BILAG index (1 patient vs 8; RR 0.1 (95% CI 0.1 to 0.9), p=0.013). SDI increase and adverse events were similar in the two treatment groups. Subgroup analyses of the primary endpoint by predefined baseline characteristics did not show evidence of a different clinical response.
Conclusion Maintenance of long term 5 mg prednisone in SLE patients with inactive disease prevents relapse.
Trial registration number NCT02558517; Results
- systemic lupus erythematosus
- treatment
- corticosteroids
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Little data are available on glucocorticoid (GC) withdrawal for patients with systemic lupus erythematosus (SLE) once remission has been achieved.
What does this study add?
In SLE patients with quiescent disease and stable treatment regimen for at least 1 year, withdrawal of 5 mg of prednisone was associated with a fourfold increase in the risk of flare.
No worsening of Systemic Lupus International Collaborating Clinics damage index and the GC toxicity index were observed during the study.
How might this impact on clinical practice or future developments?
There is an interest of continuing 5 mg prednisone at long course to avoid relapse in SLE.
Introduction
Systemic lupus erythematosus (SLE) is a chronic disease characterised by a fluctuating disease course. Glucocorticoids (GCs) play a central role in the treatment of active SLE but little data are available on GC withdrawal for patients once remission has been achieved.1–4 Although there is general agreement on the toxicity of GCs and the need to avoid long-term administration of these drugs, a significant proportion of treating physicians prefers to continue low-dose GCs despite clinical remission, particularly if there is a history of major organ involvement such as lupus nephritis or neuropsychiatric SLE.5 Observations of SLE cohorts reported that between 57% and 86% of patients undergo long-term low-dose GCs treatment.6 7
However, although some authors feel that withdrawal of low-dose GC may lead to severe flares, even after very long intervals of complete quiescence; this concept can neither be proved nor refuted based on the literature. Conversely, some studies suggest that sustained low doses of GCs might be harmful and could be associated with the accrual of irreversible organ damage over time.8–11 Accordingly, in the recent update of European League Against Rheumatism (EULAR) recommendations for the management of SLE during chronic maintenance treatment, GCs should be, when possible, withdrawn.2
Due to the lack of experimental evidence to justify long-term use of low-dose GC administration in SLE, we have conducted the CORTICOLUP study, a monocentric, 12-month, superiority, open-label, randomised controlled clinical trial comparing maintenance versus withdrawal of 5 mg/day prednisone for the prevention of flares in SLE patients with clinically inactive disease and a stable SLE treatment for at least 1 year.
Patients and methods
The study was conducted from January 2014 to April 2018 in the Department of Internal Medicine 2, French National Reference Center for SLE, Pitié-Salpêtrière Hospital, Paris, France. Written informed consent was obtained from all participants.
Patient eligibility, enrolment, randomisation and treatment
Eligible patients were 18 years or older, with a diagnosis of SLE according to the revised American College of Rheumatology classification criteria12; a clinically quiescent SLE for at least 1 year defined as: (1) SELENA-SLEDAI score ≤4,13 14 (2) D or E British Isles Lupus Assessment Group (BILAG) 200415 16 scores in all organ systems except for the haematological system, for which a C score due to leucopenia, lymphopenia or isolated positive Coombs’ test was tolerated and (3) Physician’s Global Assessment=013 14 and a treatment regimen including prednisone 5 mg/day. Prednisone, antimalarials and/or immunosuppressive therapy had to be stable for at least one consecutive year before inclusion. Exclusion criteria were patients who were pregnant, who planned a pregnancy and who were unable to sign the informed consent. Prolonged clinically quiescent SLE was defined as a 5-year consecutive period of no clinical signs of disease activity, irrespective of occurrence of leucopenia, SLE treatment and serological activity (presence of anti-double-stranded DNA (anti-dsDNA) antibodies (Abs) and/or low complement).17
Eligible subjects were enrolled in the study and computer-randomly (1:1 ratio) assigned to continue prednisone 5 mg/day for 52 weeks or to interrupt intake the day of the beginning of the study (day 0) (http://randoweb.aphp.fr/). Patients assigned to prednisone withdrawal were given hydrocortisone 20 mg/day during 1 month to prevent adrenal failure. Other SLE treatment including antimalarial and/or immunosuppressant therapy remained unmodified during the study except in case of treatment-related side effects or SLE flare requiring treatment modifications. An isolated change in anti-dsDNA or C3, in the absence of clinical manifestations, was not indicative of an increase in SLE treatment.
Outcomes and follow-up
The primary efficacy endpoint was the proportion of patients experiencing a flare using the SELENA-SLEDAI flare index (SFI)13 14 (see online supplementary text) between randomisation and week 52.
Supplemental material
Secondary endpoints included (see online supplementary text): times to flare; proportion of patients experiencing a severe flare or a mild/moderate flare using the SFI at week 5213 14; proportion of patients experiencing a flare using the BILAG index at week 5218 19; proportion of patients experiencing a severe flare, a moderate flare or a mild flare using the BILAG index at week 5218 19; changes in serological activity (anti-dsDNA Abs and C3 levels) during 52 weeks and proportion of patients experiencing an increase in the Systemic Lupus International Collaborating Clinics (SLICC) damage index (SDI) between randomisation and week 52.20 Severe and moderate flares in the BILAG index were pooled because this type of flare typically requires the prescription of corticosteroids and/or the initiation or increase of immunosuppressant and/or specific drugs in contrast to mild flares that often require symptomatic therapy. The outcomes were adjudicated by a blinded independent committee of the intervention allocation.
Patients were evaluated at baseline and at 3, 6, 9 and 12 months and were asked to contact their physician if they developed symptoms compatible with an SLE flare after which they were promptly examined. At each visit, outcomes and adverse effects were ascertained according to a history of current symptoms and medications (see online supplementary text). Follow-up data were collected until the end of 52 weeks regardless of outcome, even for subjects who had discontinued intervention.
Statistical analysis
The sample size calculation was based on the assumption that in SLE patients with inactive disease and long-term 5 mg prednisone, the risk of relapse was estimated to be 3% and that a 15 points increase in the percentage of the proportion of flare in the prednisone withdrawal group (i.e 18% flare) was considered clinically significant. Under these assumptions, at least 62 patients would have to be assigned to each group in order to have 80% statistical power permitting to conclude that prednisone maintenance was superior to prednisone withdrawing with a two-sided type I error rate of 5%. Primary and secondary endpoints and safety analyses were analysed in the intention-to-treat principle that included all randomised patients. Qualitative variables are expressed as number (%) and quantitative parameters as the mean ± standard deviation (SD) or median (range or quartiles alternatively), as appropriate. Differences between groups of patients were tested using the Mann-Whitney test for continuous data, and Fisher’s exact test or the Khi-2 test for categorical data. Times to flare were represented by means of the Kaplan-Meier method and compared using Log-Rank tests. Hazard ratio were obtained using the Cox proportional hazards model. Interaction between treatment effect and pre-specified subgroup effect was tested using a logistic regression model. Since the variables pertaining to “disease duration” and “GCs duration” are closely linked, the former was not included in the interaction analysis. All tests were two-sided and p<0.05 defined significance statistical analyses were performed using GraphPad Prism, V.5.0 software (GraphPad Software, San Diego, California, USA) and SAS V.9.4 software.
Results
Baseline demographic and disease characteristics
A total of 124 patients were enrolled. Sixty-one and 63 patients were randomised in the prednisone maintenance and the prednisone withdrawal groups, respectively (figure 1). In the prednisone maintenance group, two patients stopped prednisone intake for personal reasons. In the prednisone withdrawal group, four patients restarted prednisone at 5 mg/day, two for personal reasons and two because of pregnancy. All patients completed the study, including its follow-up. Baseline clinical characteristics at randomisation are summarised in table 1. There were no significant differences between the two treatment groups with respect to any of the baseline clinical characteristics, except a significantly higher number of patients under methotrexate in the maintenance group (p=0.035) and under mycophenolate mofetil in the prednisone withdrawal group (p=0.038). At study entry, all patients were in ‘remission on treatment’ according to the DORIS consensus21 22 and in ‘remission on corticosteroids’ according to the Zen et al definition.23 A total number of 24 (39%) patients in the maintenance group and 32 (51%) patients in the withdrawal group were in prolonged clinically quiescent SLE.
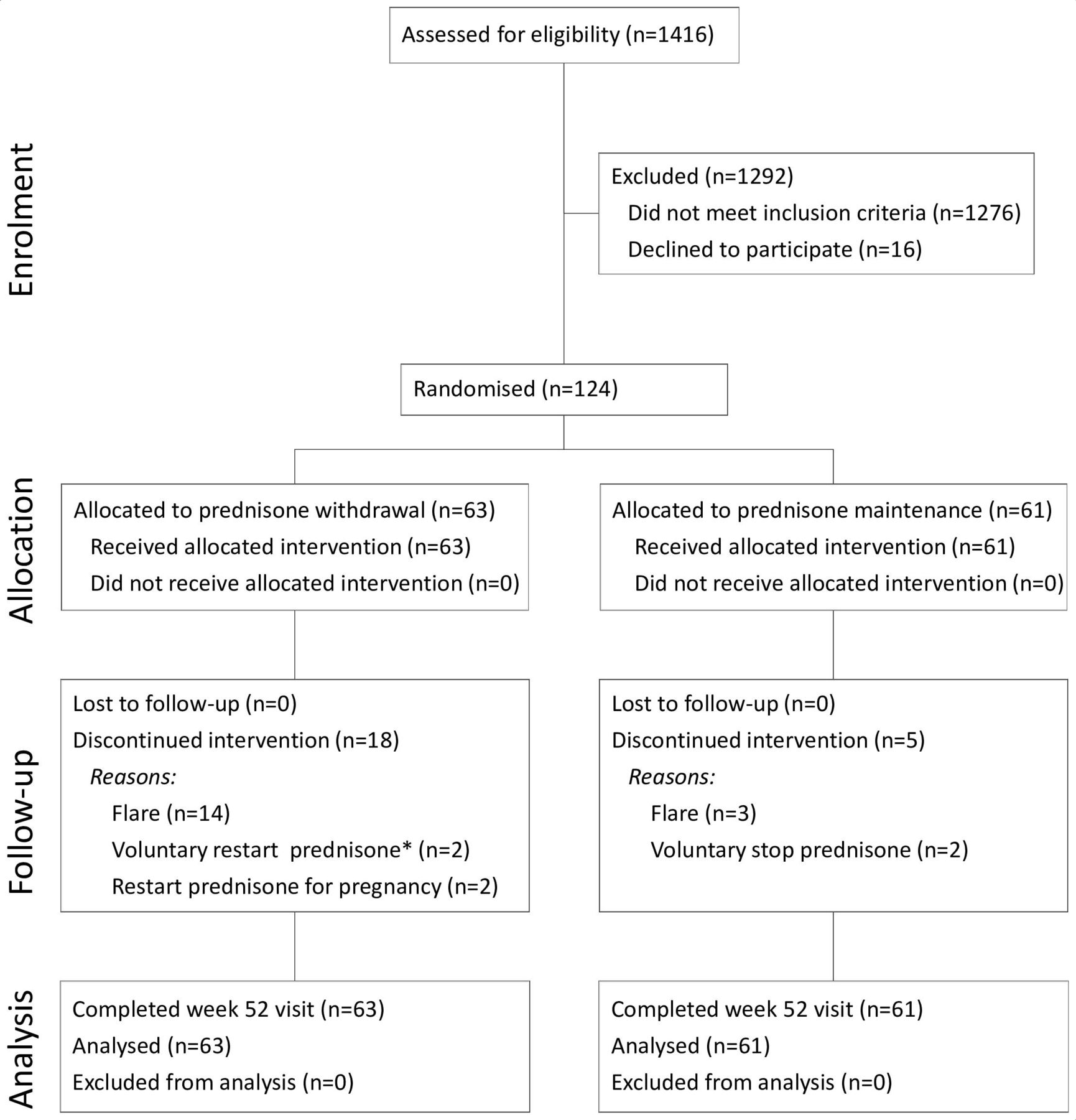
Study flow diagram. In the prednisone withdrawal allocated group, 14 patients experienced a flare that justified restart of prednisone and 4 patients restarted prednisone while not experiencing lupus symptoms (2 for pregnancy and 2 for personal reasons). In the prednisone maintenance allocated group, three patients experienced a flare that justified increase above 5 mg/day of prednisone and two patients stop prednisone 5 mg/day for personal reasons. All patients completed the 52 weeks follow-up and were included in the intention-to-treat analysis. *One patient who restarted prednisone for personal reasons became pregnant afterwards.
Baseline demographic and clinical characteristics of the study subjects
Withdrawal of low dose of prednisone increases the risk of flares in SLE patients with clinically quiescent disease
Primary endpoint
Using the SFI, the proportion of patients who experienced a flare at 52 weeks differed significantly between the two groups: 4/61 (7%) patients in the maintenance group versus 17/63 (27%) in the withdrawal group (RR 0.2 (95% CI 0.1 to 0.7), p=0.003, see table 2).
Results for primary and secondary endpoints at 52 weeks
Secondary endpoints
SLE flares
The occurrence of flare during 52 weeks is presented as a Kaplan-Meier curve of cumulative probability (figure 2). The estimated hazard ratio (prednisone maintenance/prednisone withdrawal) of flare occurrence was 0.2 (95% CI, 0.1 to 0.6, p=0.002 by log-rank).

Kaplan-Meier estimates of the cumulative probability of flare for patients in the prednisone maintenance and prednisone withdrawal groups. Clinically quiescent SLE patients were allocated at day 0 to stop (blue line) or to continue (red line) prednisone 5 mg/day and were followed for 52 weeks. Each corner in the curve represents a lupus flare, defined by SELENA-SLEDAI flare index. Patients who had a flare in any organ system were recorded. Kaplan-Meier plots show the percentage of patients who flared in any organ system. All patients had a 52 weeks survey. No patient was censored before the end of the study. Curves were compared using log-rank tests. Crude HR was calculated using a proportional risk COX model. Pred, prednisone; SLE, systemic lupus erythematosus.
When recording flares using the BILAG index, the proportion of patients who experienced a flare at 52 weeks differed significantly between the two groups: 4/61 (7%) patients in the maintenance group versus 17/63 (27%) in the withdrawal group (RR 0.2 (95%CI 0.1 to 0.7), p=0.003, see table 2).
Analysis of flare severity at 52 weeks using the SFI showed a significantly lower proportion of mild/moderate flare (3 patients vs 12; RR 0.2 (95% CI 0.1 to 0.8), p=0.012) and a non-significant lower proportion of severe flare (1 patient vs 5; RR 0.2 (95% CI 0.1 to 1.5), p=0.096) in the maintenance group, as compared with the withdrawal group. Flare severity analysis using the BILAG index assessment showed a significantly lower proportion of moderate/severe flare in the maintenance group as compared with the withdrawal group (1 patient vs 8; RR 0.1 (95% CI 0.1 to 0.9), p=0.013).
The clinical manifestations and treatment of flares are depicted in table 3. There were 4 cases of arthritis, 2 cutaneous manifestations, 1 class V lupus nephritis and 1 mucosal ulcer in the maintenance group and 12 arthritis, 7 cutaneous manifestations, 2 class V lupus nephritis, 1 mucosal ulcer, 1 pericarditis, 1 catatonia, 1 cranial neuropathy and 1 thrombocytopenia in the withdrawal group. In the prednisone maintenance group, three flares were treated with prednisone above 5 mg/day and one with the start of an immunosuppressant drug. In the prednisone withdrawal group, 12 flares were treated with prednisone above 5 mg/day and 4 with a new immunosuppressant or immunomodulatory drug. To be certain that an adrenal insufficiency was not misdiagnosed as a lupus flare, four patients with less evident symptoms of synovitis and arthritis underwent a short Synacthen test that revealed no diagnosis of adrenal insufficiency (online supplementary table S1).
Clinical manifestations and treatment of flares according to treatment group
Damage accrual
Four items of the SDI were scored during 52 weeks in a total of three patients in the prednisone withdrawal group: two osteoporosis-related fractures, one retinal toxicity due to antimalarials and one cataract. No damage-related events were recorded in the prednisone maintenance group. The proportion of patients who experienced an increase in the SDI was similar between the two groups (table 2).
Changes in immunological parameters
The anti-dsDNA Ab and C3 serum levels, as well as the proportion of patients with positive anti-dsDNA Abs and those with low C3, did not significantly change during 52 weeks in either group (online supplementary figure S1 and data not shown).
Risk of flare in patients’ subgroups
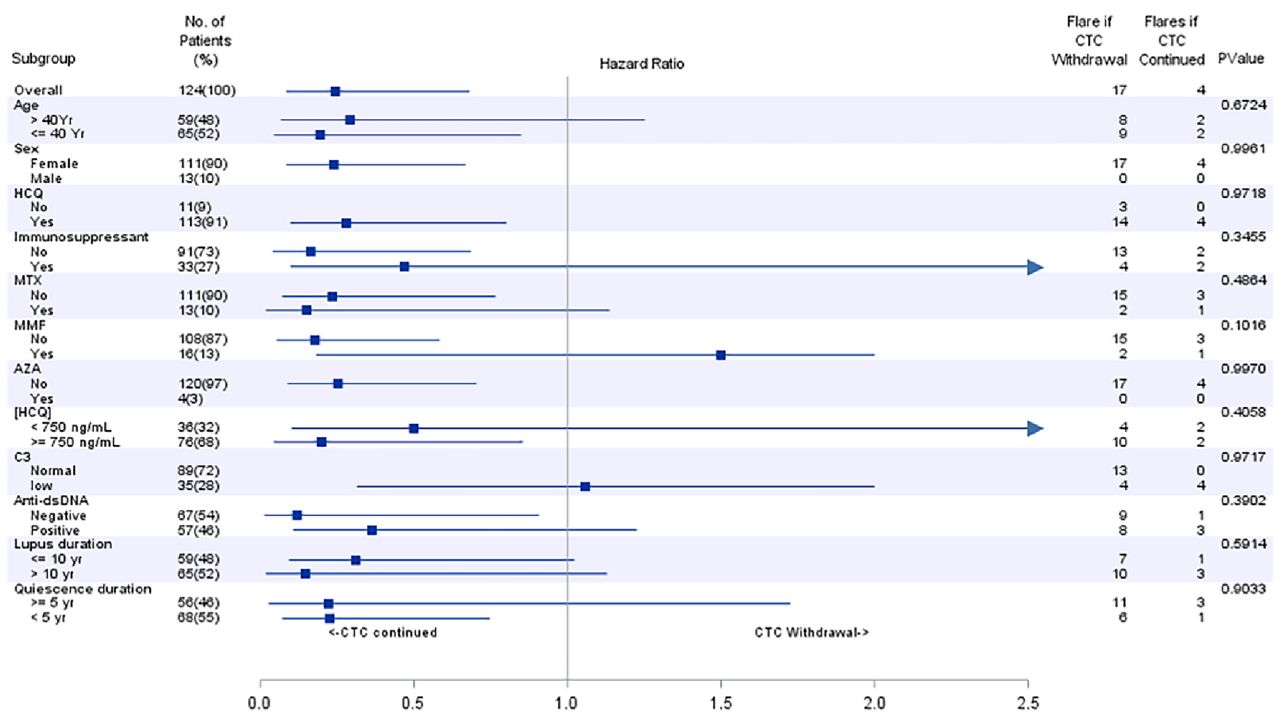
The effect of treatment maintenance was consistent among prespecified subgroups (figure 3).

{kind=link}
{kind=link}
{kind=link}
Risk of flare in patients subgroups. The impact of maintenance or withdrawal of prednisone on the occurrence of lupus flare was studied according to predefined subgroups. The HR was derived from a COX model, with treatment as the only factor, according to subgroup. AZA, Azathioprine; C3, complement fraction 3; dsDNA, double-stranded DNA; HCQ, hydroxychloroquine; [HCQ], blood concentration; MMF, mycophenolate mofetil; MTX, methotrexate.
Adverse events
During the 52 weeks of the study, adverse events (table 4) were rare in both groups. There were no deaths, no vascular thrombosis, no malignant neoplasm and no adverse events that required the discontinuation of prednisone or hospital admission. Six patients, three in each group, became pregnant during the study. In a post-hoc statistical analysis, the mean±SD variation of the composite glucocorticoid toxicity index (GTI) between baseline and month 12 was similar in the maintenance (3.3±13.0) and the withdrawal groups (3.7±16.5) (p=0.9). The proportion of patients who experienced a worsening in their composite GTI between baseline and month 12 was also similar in the two groups (23% vs 29%, p=0.5).
Adverse events by treatment group
Discussion
Understanding the benefits and risks of long-term maintenance of low-dose GCs is an important consideration in the care of SLE. The present study prospectively shows that in SLE patients with quiescent disease and stable treatment regimen for at least 1 year, withdrawal of 5 mg of prednisone was associated with a fourfold increase in the risk of flare, as defined by the SFI or the BILAG index, thereby emphasising the interest of continuing a low dose of prednisone at long course to avoid relapse.
GCs tapering and withdrawal are considered one of the main targets of SLE management, but at present the decision of withdraw GCs is left to the judgement of the treating physician. A recent internet-based survey of 130 clinicians from 30 countries showed that preference of clinicians in treatment reduction in patients with SLE in clinical remission was variable with greater caution in treatment reduction when patients have persistent serological abnormalities and previous major organ involvement.5 Prednisolone was by far the first medication that physician suggested reducing or withdrawing during remission, irrespective of persistent serological abnormalities, remission duration, minor or major organ involvement and whether prednisolone was used with hydroxychloroquine (HCQ) alone or as part of a regimen also involving HCQ and an immunosuppressant.5 To our knowledge, the present study is the first randomised controlled trial comparing the risk of relapse after withdrawal of low-dose prednisone in clinically quiescent SLE. Galbraith et al have undertaken a pilot trial comparing continuation and withdrawal of 7.5 mg of prednisone in SLE patients with a history of previous lupus nephritis but this trial was designed to study the feasibility of a larger trial and not to assess the efficacy and safety of this treatment intervention.24 However, there is some indirect data that underscore the importance of low-dose GCs for maintaining clinical quiescence. Indeed, it is well known that prolonged complete remission defined by the absence of clinical activity with no use of GCs and immunosuppressant is infrequent in SLE ranging from 2% to 32%.11 17 23 25–27
The 27% relapse rate observed in the withdrawal group in our study is in line with the ones recently reported in two recent cohorts.28 29 Tani et al described the longitudinal study of a cohort of 91 SLE Italian patients who attempted GC stopping.28 A total of 77 patients successfully stopped GC. For those patients who were successfully withdrawn from GC, 18 flares (23%) were recorded after a median follow-up period of about 2 years.28 Like in our study, 72% of flares were mild. The time period since the last flare was the sole determinant predictor of disease flare identified.28 Goswami et al in a recent observational study preformed in India reported that 21% of patients in remission undergo exacerbation of the disease after GC withdrawal with most of the flares occurring in the first year of follow-up.29 Unlike our study, many flares were deemed major. Furthermore, Goswami et al defined duration of disease, duration of GCs before interruption and second immunosuppressive as independent predictors of flare-free survival,29 whereas in our prospective randomised study none of the above-mentioned factors was associated with the risk of flare after GC withdrawal. However, we cannot completely rule out certain associations since subgroups analyses were performed only on relatively small size samples. In particular, the results might have been different should the majority of patients have been treated with an immunosuppressant.
In other autoimmune diseases, there is evidence that low-dose long duration of GC use is beneficial. A systematic review and meta-analysis of prednisone withdrawal in ANCA-associated vasculitis found that late continuation of prednisone was associated with a twofold reduction of the frequency of relapses.30 Moreover, in rheumatoid arthritis, the results from two randomised, controlled trials have shown that continuation of low-dose GC provided better disease control than GC withdrawal.31 32 Yet, these results have to be interpreted with caution given the different pathogenesis of these autoimmune diseases.
The interpretation of maintaining low-dose prednisone therapy is subject to prudence, since the CORTICOLUP study has not been able to prove that maintaining low-dose steroids would diminish damage accrual in a statistically significant way. However, the reduction in the number of flares with the maintenance of prednisone at low doses is clearly important because previous reports have shown a strong link between the number of flares and the damage accrual, as well as the quality of life.33–36 Enthusiasm for long-term prednisone, even if effective, is also tempered by potential side effects such as infections, diabetes mellitus, cataract, osteoporosis, gastrointestinal bleeding and cardiovascular disease, leading to the development of irreversible organ damage.7 9 10 37–42 Even if some studies suggest that sustained low doses of GCs might be harmful and could be associated with the accrual of irreversible organ damage over time,8–11 a recent report from the EULAR agreed that the level of harm conveyed by long-term GG administration is dose-dependent with dosages of ≤5 mg/day prednisone producing an acceptably low level of harm, with the exception of patients at high cardiovascular risk who may require preventive measures.43 In line with these data, we observed a low SDI score on CORTICOLUP inclusion and no worsening of SDI and GTI scores during the study. However, the small number of patients included and the limited monitoring time prevent us from drawing any meaningful conclusion on the tolerance of long-term prednisone maintenance.
The results of the study should be interpreted in light of its limitations. First, it was an open-label trial without a placebo group. However, given that outcomes were strictly adjudicated by an independent assessor, they are unlikely to be affected by knowledge of patient allocation. Second, this study was a monocentric investor-led clinical trial: nevertheless, patients were educated to detect signs of flare and contact their physicians and no patients were lost to follow-up. Third, although in this study no data on ethnicity are given, it has to be noted that the French population of SLE patients is widely multi-ethnic, and includes a significant proportion of patients from African and Asian ancestors. Fourth, because withdrawal of 5 mg of prednisone was relatively abrupt, we cannot exclude that slow prednisone tapering would have resulted in less flares. However, there is no experimental data in SLE sustaining this hypothesis. Of note, in a recent randomised, controlled trial with rheumatoid arthritis patients with a low disease activity status, it was found that continued prednisone-equivalent dose 5 mg provided better disease control than GC withdrawal, even if the latter was slowly tapered in monthly 1 mg decrements.44 This study confirms two previously published reports with a close design.31 32 Fifth, it can be argued that certain cases of lupus flares in the withdrawal group might have been misdiagnosed as adrenal insufficiency because cortisol levels were not systematically assessed during the study. However, the occurrence of events such as rash, alopecia, arthritis, synovitis, serositis and nephritis cannot be confused with symptoms of adrenal insufficiency. Furthermore, other signs of adrenal insufficiency such as gastrointestinal symptoms, hypoglycaemia, hypotension, hyponatremia, lymphocytosis and hypereosinophilia were absent as well. Therefore, the clinical and laboratory manifestations observed in patients who have discontinued corticosteroid therapy were clearly those of SLE. Finally, it is possible that our study may suffer from an inclusion bias. The SLE patients were kept on low dose of steroids by their treating physician despite clinical remission. It is possible that these patients have a special lupus history with severe flares, major organ involvements and relapses that prompted the physician to maintain this long-term treatment. Thus one must be circumspect in extrapolating the results to all SLE patients in remission. The results should also be interpreted in the context of approximately three-quarters of patients experiencing GC withdrawal success.
In conclusion, despite some limitations, our study presents to date the strongest evidence that maintenance of 5 mg prednisone is superior to its withdrawal in order to prevent flares in SLE patients in remission. These results must be validated in other independent cohorts and larger studies must be undertaken to determine whether clinical characteristics and new biomarkers, such as elevated serum interferon alpha levels, could help clinicians to identify a subgroup of SLE patients clinically in remission but who are at higher risk of relapse and who would benefit from a continued intake of low doses of prednisone.
Acknowledgments
We thank the patients, the nurses and the staff of the Department of Internal Medicine 2 who participated in this study. We thank Professor Anne Bachelot (Sorbonne Université, Assistance Publique–Hôpitaux de Paris, Groupement Hospitalier Pitié–Salpêtrière) for her advices.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Lay summary
Disclaimer : This is a summary of a scientific article written by a medical professional (“the Original Article”). The Summary is written to assist non medically trained readers to understand general points of the Original Article. It is supplied “as is” without any warranty. You should note that the Original Article (and Summary) may not be fully relevant nor accurate as medical science is constantly changing and errors can occur. It is therefore very important that readers not rely on the content in the Summary and consult their medical professionals for all aspects of their health care and only rely on the Summary if directed to do so by their medical professional. Please view our full Website Terms and Conditions.
Copyright © 2020 BMJ Publishing Group Ltd & European League Against Rheumatism. Medical professionals may print copies for their and their patients and students non commercial use. Other individuals may print a single copy for their personal, non commercial use. For other uses please contact our Rights and Licensing Team.
Footnotes
Handling editor Josef S Smolen
AM and MP contributed equally.
Contributors AM, MP, HD and ZA contributed to the conception and design of the study; AM, MP, JH, FC-A, MH, MPdC, THDB, MM, GG, PC and ZA were involved in the acquisition of data; AM, MP, JH, FC-A, MH, MPdC, THDB, MM, GG, HY, PC, HD and ZA contributed to the analysis and interpretation of data. All authors contributed to drafting and/or revising the manuscript.
Funding This work includes independent financial support by the Assistance Publique–Hôpitaux de Paris (AP-HP), Institut National de la Santé et de la Recherche Médicale (Inserm) and Sorbonne Université.
Competing interests Professor Devilliers reports personal fees from Johnson & Johson, personal fees from GSK, grants from LFB, non-financial support from Novartis, non-financial support from MSD, outside the submitted work
Ethics approval The study protocol was approved by the Comité de Protection des Personnes (CPP) EST I (Dijon). The study was conducted in accordance with the ethical principles of the Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.