Article Text

Abstract
Objectives To evaluate the annual direct medical cost of managing adult systemic lupus erythematosus (SLE) patients with active autoantibody positive disease in Europe.
Methods A 2-year, retrospective, multicentre, observational study was conducted in five countries (France, Germany, Italy, Spain and the UK). Data included patients’ characteristics, disease activity and severity, flare assessments and health resource use (eg, laboratory tests, medications, specialist visits and hospitalisations). Costs were assessed from the public payers’ perspective. Cost predictors were estimated by multivariate regression models.
Results Thirty-one centres enrolled 427 consecutive eligible patients stratified equally by disease severity. At baseline, mean (SD) age was 44.5 (13.8) years, 90.5% were women and mean (SD) SLE duration was 10.7 (8.0) years. The SELENA-SLEDAI (11.2 vs 5.3) and SLICC/ACR index (1.0 vs 0.7) scores were higher in severe patients. Over the study period, patients experienced on average 1.02 (0.71) flares/year. The mean annual direct medical cost was higher in severe compared to non-severe patients (€4748 vs €2650, p<0.001). Medication costs were €2518 in severe versus €1251 in non-severe patients (p<0.001). Medications represented 53% and 47% of the total cost for severe and non-severe patients, respectively, primarily due to immunosuppressants and biologics. Flares, especially severe flares, were identified as the major cost predictor, with each flare increasing the annual total cost by about €1002 (p<0.001).
Conclusions The annual direct medical cost of SLE patients in Europe is related to disease severity and flares. Medical treatments were the main cost drivers. Severe flares and major organ involvement were identified as important cost predictors.
- Systemic Lupus Erythematosus
- Disease Activity
- Autoantibodies
- Economic Evaluations
- Autoimmune Diseases
Statistics from Altmetric.com
Introduction
Systemic lupus erythematosus (SLE) is a multi-organ, autoimmune disease characterised by alternating periods of disease activity and remission. Numerous organs may be affected (skin, joints, lungs, heart, kidneys and brain) leading to a wide combination of clinical manifestations.1 ,2
Patients may receive several drug combinations including corticosteroids, non-steroidal anti-inflammatory drugs (NSAIDs), antimalarials and immunosuppressive/cytotoxic drugs.3–5 In recent years, biological agents, especially rituximab, have been widely used in Europe as an off-label treatment in patients with refractory disease.6 ,7
Several studies show that SLE imposes a substantial economic burden on the healthcare system and on society, due to both direct and indirect costs.8–13
Data on SLE costs are available for Asia, Europe and North America, but are very limited and/or outdated for Europe. A tri-nation study, in the UK, Canada and the USA,14–16 evaluated the costs of treating SLE patients over a 4-year follow-up period. Applying Canadian unit costs, Sutcliffe et al17 reported the costs for 105 patients assessed over a 4-month period in the UK, while Huscher et al11 estimated the costs for 844 patients over 12 months in Germany.
It has recently been highlighted that little research has been conducted which examines variations in costs associated with disease activity, severity, disease manifestations or with specific treatments.18
The aim of this study was to evaluate the annual direct medical cost for adult SLE patients with active, autoantibody positive disease, and to identify the cost drivers (eg, medications) and predictors (eg, flares) in five European countries (France, Germany, Italy, Spain and the UK).
Patients and methods
Study design
The LUpus erythematosus Cost of Illness in Europe study (LUCIE) is a 2-year multi-centre, retrospective study based on data reported in patients’ medical records. The study was carried out in France, Germany, Italy, Spain and the UK, in 26 hospital and five office-based practices (in Germany, to reflect the national specific management of SLE), from October 2010 to April 2011.
In each country between four and 10 centres specialising in SLE management enrolled between five and 50 SLE patients with active, autoantibody positive disease. SLE disease was considered active in the presence of one of the two following criteria: (1) one change in treatment related to SLE activity (increase in dose and/or new treatment) and/or the occurrence of a new manifestation or worsening of clinical symptoms of SLE; or (2) one positive biomarker of SLE activity (anti-dsDNA antibodies and/or C3 or C4 below normal) and one clinical and/or haematological feature of SLE.
Each country enrolled 50% severe and 50% non-severe patients. Severe patients were defined as having at least one major domain involved at inclusion (renal, neurological, cardiovascular or respiratory) and requiring prednisone equivalent dosages >7.5 mg/day and/or immunosuppressants. Patients’ disease activity and severity were assessed at baseline.
Patients who met the inclusion criteria were pre-selected for inclusion into the study. Patients were screened between January and June 2008 to identify the inclusion visit where the patient met the eligibility criteria (figure 1).

Design of the study.
The study followed the local legal requirements. It was approved by the local ethics committees in Germany, Italy and the UK, where informed consent was obtained from each patient, and by the national regulatory authorities in France and Spain.
Disease activity and organ damage assessment
Disease activity and organ damage were evaluated retrospectively at baseline using the SELENA-SLEDAI instrument19 and the SLICC/ACR index,20 respectively.
Definition, identification and severity of flares
Flare occurrence and its severity were defined by treatment changes (ie, increasing dose of corticosteroids and/or initiating a new SLE treatment) and/or hospitalisation, based on an adaptation of the SELENA-SLEDAI flare index.21 It was not possible to identify the end of a flare. In the event of two consecutive flares, the second one was considered to be a new flare if it occurred more than 60 days after the beginning of the first one.
Healthcare resource evaluation and cost calculation
The direct annual medical costs were assessed for each country from the public payers’ perspective. The units of resource use were converted in monetary costs using the local official unit cost databases available in 2011 (see online supplementary table S1).
Information on all resources used (medications, laboratory tests, biopsies, imaging tests, specialist visits and hospitalisations) was collected from the medical records for each patient over the 2-year follow-up study period.
Costs were first calculated for each patient. Unit costs were attributed to each unit of medical resource per category. Then for each resource category the costs of the overall study sample were pooled and divided by the corresponding number of patients. Total direct costs were calculated for each patient over the follow-up study period and expressed as an annual value taking into account the individual number of months of follow-up.
An ancillary study was conducted in nine centres (three per country) in France, Italy and Spain to evaluate the distribution of disease severity (severe and non-severe patients) of the overall SLE population. Results were applied to the study sample to ensure that the costs were representative of the active SLE population.
Statistical analysis
Statistical analysis was performed using SAS V.9.1 (SAS Institute Inc, Cary, North Carolina, USA) under the Windows operating system.
All variables were analysed independently at the country level and then for the entire study sample. Data were analysed on the entire sample and also stratified by disease severity (severe vs non-severe).
The two-sample t test or Mann-Whitney test was used for quantitative variables and the χ2 test or Fisher's exact test for qualitative variables. Statistical significance was set at 0.05.
Cost predictors associated with annual direct medical costs were identified using multivariate regression models. Annual direct medical costs (dependent variable) were normalised using a logarithmic transformation. Univariate regression models were performed for each independent variable and a p value threshold of 0.1 was applied for selecting variables for inclusion in the multivariate model and assessing the possible colinearity between selected independent variables. The backward selection method was used to determine the best fitting model to predict annual direct medical costs. In addition, in order to assess and explain possible differences between countries, the variables indicating each of the five European countries were included in the model with the UK serving as the reference country.
Results
A total of 427 eligible patients, consisting of 212 severe (49.6%) and 215 non-severe (50.4%) patients, were included in the analysis. Ten patients were excluded because of non-compliance with eligibility criteria (see online supplementary figure S1). The mean (SD) follow-up study duration was 24.7 (3.2) months.
Baseline characteristics
Table 1 reports the baseline demographics and clinical characteristics of patients.
Baseline characteristics: patient demographics and clinical profile
Patients’ mean (SD) age was 44.5 (13.8) years, 90.5% were women, 84.5% were Caucasian, 10.6% were black, 3.0% were Central/South Asian and 1.8% were East/South East Asian or other. (Data on ethnicity were not collected in France because of ethics considerations.) Mean (SD) SLE duration was 10.7 (8.0) years.
Disease activity and organ damage
The mean (SD) SELENA-SLEDAI score was 8.2 (6.7), and twice as high in severe compared to non-severe patients (p<0.001) (table 1). The disease was most active in major organs, and in severe patients. The proportion of major organs involved in severe patients was 6, 12 and 30 times higher than in non-severe patients (p<0.001 each) for the renal, cardiovascular/respiratory and neurological systems, respectively.
The mean (SD) SLICC/ACR index score was 0.8 (1.4) and was also higher in severe patients (p=0.010). Notably, 50.0% of severe versus 33.5% of non-severe patients (p<0.011) had at least one damaged organ. The proportion of major organ damage in severe patients was 5.3 times higher (p<0.001) for renal and 2.2 times higher (p<0.01) for neuropsychiatric systems than in non-severe patients.
Antibodies and complement
ANA, anti-dsDNA, anti-ENA and anti-phospholipid antibodies were positive, respectively, in 97.1%, 70.8%, 63.5% and 43.6% of patients. C3 and C4 were below normal in 45.0% and 50.0% of patients. In severe patients, biomarkers related to disease activity were more frequently impaired: anti-dsDNA (77.6% vs 63.6%, p<0.01), C3 (53.1% vs 36.6%, p=0.003) and C4 (57.1% vs 42.7%, p=0.02).
Analysis of flares
Most patients (87.6%) had a flare at least once over the study period (see online supplementary table S2). Twice as many severe patients experienced severe flares compared to non-severe patients (71.2% vs 34.4%, p<0.001).
The mean (SD) annual number of flares was 1.02 (0.71), consisting of 0.54 mild/moderate and 0.47 severe flares. Severe patients had more frequent flares compared to non-severe patients (1.13 vs 0.91 flare, p=0.001) and were more likely to experience severe flares (0.70 vs 0.25 flare, p<0.001).
The mean (SD) annual number of severe flares requiring hospitalisation was 0.25 (0.52), which was also higher in severe patients (0.36 vs 0.14, p<0.001).
Patients experiencing flares were most commonly treated with either corticosteroids (94.3%), antimalarials (68.1%) or immunosuppressants (67.5%). Immunosuppressants (81.8% vs 54.9%, p<0.001) and biologics (10.5% vs 1.7%, p<0.001) were more often prescribed for treating severe flares compared with mild/moderate flares. Both drugs were frequently used in combination with corticosteroids (see online supplementary table S3).
Direct medical cost
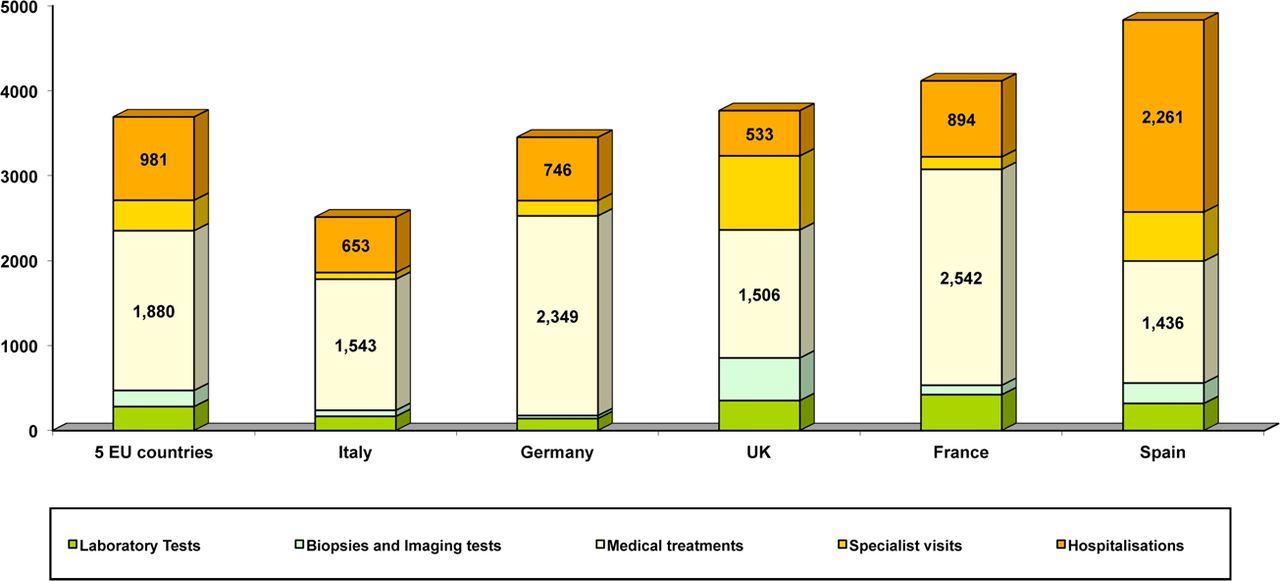
The mean annual direct medical cost of treating severe patients was 1.8 times higher than non-severe patients (€4748 vs €2650, p<0.001; table 2). A very wide range of costs was observed in both groups (from €117 to €37 130). The mean (SD) annual direct medical cost of the study population was €3691 (€4411) which ranged from €2513 to €4833 in the five countries (figure 2).

{kind=link}
{kind=link}
Cost of each category of health resource use (in €), globally and in the five countries.
Mean annual direct medical cost of active SLE patients by disease severity
The ancillary study included 738 patients among whom 228 fulfilled the main study inclusion criteria (ie, with active autoantibody positive disease, on medication for SLE). Among the patients with active disease, 39.7% had severe and 60.3% non-severe disease. Data from this ancillary study were used to estimate the mean annual adjusted direct cost per patient of €3483, which was 5.6% lower than the unadjusted cost. The adjusted costs in the five countries were as follows: €2549 (Italy), €3067 (Germany), €3651 (UK), €4003 (France) and €4156 (Spain).
Healthcare resource use and associated mean annual direct costs
Table 3 reports the costs of medical resources used by the patients in the study.
Description of annual direct medical cost of active SLE patients by disease severity
Medications (€1880), hospitalisations (€981), investigative tests (€472) and specialist visits (€359) represented 50.9%, 26.6%, 12.8% and 9.7%, respectively, of the estimated annual total medical cost.
Medications
Over the study period, 92.7% of patients received corticosteroids, 75.6% antimalarials, 72.6% immunosuppressants, 24.1% NSAIDs, 10.3% biologics and 60.4% anti-osteoporosis drugs (see online supplementary table S4). Severe patients were more frequently prescribed corticosteroids (97.6% vs 87.9%, p<0.001), immunosuppressants (88.7% vs 56.7%, p<0.001) including mycophenolate mofetil (59.9% vs 24.6%), and biologics (15.1% vs 5.6%, p=0.001).
The mean annual cost of medications for severe patients was €2518, twice as high as for non-severe patients (€1251, p<0.001). Medications were the main cost driver, representing 53.0% and 47.2% of the total cost of care for severe and non-severe patients, respectively (table 3).
The costs of immunosuppressants and biologics were 2.9 and 2.7 times higher in severe compared to non-severe patients, respectively (p<0.001 each). The mean annual cost of immunosuppressants and biologics represented 28.8% and 6.8% of the total cost, respectively.
Among the five countries, the mean annual cost of treatments ranged from €1436 (Spain) to €2542 (France), and represented from 29.7% (Spain) to 68.1% (Germany) of the total medical cost (figure 2).
Hospitalisations
During the study period, 43.1% of patients were admitted to hospital at least once on an inpatient basis and 22.5% on a day basis. Inpatient admissions (54.2% vs 32.1%, p<0.001) and day hospitalisations (26.9% vs 18.1%, p=0.030) were higher for severe patients. Inpatient admissions to intensive care and rehabilitation units occurred in seven and 11 cases of severe and non-severe disease, respectively. While hospitalisations accounted for the same relative percentage (26–27%) of the total direct costs for severe and non-severe patients, the absolute cost for severe patients (€1247) was almost twice that of non-severe patients (€718) (table 3). The mean cost of hospitalisations for severe patients was almost twice that of non-severe patients (p<0.001).
Specialist visits
Over the study period, 70.7% of patients consulted a rheumatologist (the primary SLE care management physician in Italy, Germany and the UK). One third of patients consulted an ophthalmologist (34.9%) or an internist (37.7%). Other specialists, such as nephrologists (14.8%) and dermatologists (13.6%), were consulted by less than 15% of the patients. Only nephrologists were 3.2 times more frequently consulted by severe patients (22.6% vs 7.0%, p<0.001). The mean cost of specialist visits was similar in the two groups of patients.
Laboratory tests
Over the study period, all patients had at least one laboratory test. Biopsies were conducted in 18.3% of patients, more frequently in severe than in non-severe patients (27.8% vs 8.8%, p<0.001). Imaging tests were conducted in 65.8% of patients, more frequently in severe than in non-severe patients (72.6% vs 59.1%, p<0.01).
The mean annual costs of laboratory tests, biopsies and imaging tests were higher in severe patients than in non-severe patients (p<0.001 each), representing 7.7%, 2.0% and 3.2% of the total cost, respectively (table 3).
Predictors of costs
The univariate regression models tested and identified the variables used in multivariate models (see online supplementary table S5). The multivariate regression models identified cost predictors on the study sample (table 4).
Results of the multivariate regression models
The occurrence of flares during the study period also resulted in an average increment in the annual cost of 35.0% (+€399, p=0.03), as compared to the cost of patients with no flares. The strongest predictor of total costs was the annual number of severe flares, with each severe flare resulting in a 97.4% (+€1002, p<0.0001) increase in the annual cost of SLE. Other important predictors of costs included major organ involvement, resulting in incremental cost increases of 25.9–52.2% when the following systems were involved: cardiovascular/respiratory (+€596), renal (+€511), neurological (+€495) and haematological (+€281). There were no significant differences related to the specific countries where patients were treated.
Discussion
The LUCIE study provides data on the healthcare resource utilisation and the direct medical costs of SLE management in Germany, the UK, France, Italy and Spain. It included patients with active disease and focused on the effect of disease severity, organ involvement and treatments on the direct medical costs of SLE.
To our knowledge, this is the first time such data have been available for France, Italy and Spain. Moreover, the study provides an update on the cost of SLE care in Germany and the UK.11 ,17 ,22
The demographic characteristics of patients were similar to those reported in other European and international studies.10 ,11 ,15 ,17 ,23 ,24 The mean direct annual costs, assessed in the five countries and overall (€3483), were consistent with those published in the two other European studies, which ranged from €342117 to €363611 (€2009). However, it is difficult to compare the direct annual costs of SLE obtained in this study with those in previous European studies as they were conducted more than 10 years ago, before the widespread use of biologics,11 ,17 and one study was conducted from a societal perspective.11 It is even more difficult to compare the costs reported in North American studies with those in Western European studies as the costs of SLE reported in the USA are 2.8 to four times higher (range: €9834–14 873 in €2009[23, 24]). Differences can be attributed to variation in disease severity profiles, study designs, healthcare systems, cost and relative prices.
Cost drivers and predictors identified in the literature were: younger patients,9 ,17 high disease activity at onset9 ,10 or over the disease course,10 ,17 flares, particularly major organ flares,10 greater disease damage,9 ,16 and disease severity including the type of organ involvement, especially active glomerulonephritis12 ,16 ,23 ,25–27 and neuropsychiatric involvement.28
This study shows that high disease severity and disease flares increase the total medical cost.
The highest costs of SLE management are related to major organ involvement (renal, neurological, cardiovascular and/or respiratory domains) and consequently to severe disease. Medications, especially immunosuppressants and biologics, were more often prescribed in severe patients and to treat severe flares. They represented approximately half of the costs and were identified as the main cost drivers, especially for immunosuppressants and biologics. The costs of medications were twice as high as those described in previous European studies, where they represented 17.3% (€592)17 and 26.6% (€967)11 of the total cost. However, these European studies were conducted more than 10 years ago and did not use biologics, which were used in our study and explained 6.8% of the annual total cost. In the last few years, SLE recommendations and care management have changed,3–6 especially with regards to the use of biologics.
The costs of SLE medications had the widest range (€247–2527; €2009) in the US studies, representing from 4.0%28 to 25.7% of the total cost.23 ,24
In addition, one major difference between our study and the others is probably the high disease activity of our patients, observed especially in severe patients, who required high doses of medications and/or immunosuppressive treatments. Notably, the use of mycophenolate mofetil, the most expensive immunosuppressant, has increased in the last few years.12
The highest costs are related to the number of severe flares, and thus to disease activity. Severe flares, which required hospitalisation in 25% of cases, were identified as the major cost predictors. Actually, the annual mean number of flares was similar to that reported in two recent studies in patients who experienced flares.10 ,28 As in our study, the direct cost of these patients with severe (renal/neuropsychiatric) flares was higher compared to those with no flares.10 ,28
The LUCIE study has a number of limitations. A 50 : 50 division between severe and non-severe patients was chosen in order to have enough power to analyse these two subgroups. The ancillary study results demonstrate that the adjusted mean cost is only 5.6% lower than the unadjusted cost. Patients’ disease severity and activity profile were assessed only at baseline. Consequently, the potential for disease progression during the 2-year follow-up period was not measured. In addition, the 2-year study duration did not allow damage accrual and the long term effects of the disease and the medications to be captured. Due to the retrospective nature of the study, the evaluation of direct medical costs may be underestimated because it was not possible to capture all components of the direct medical costs (eg, non-specialist visits and treatments associated with SLE comorbidities, antibiotics). Finally, as there is no generally accepted definition of a lupus flare, it was necessary to define specific criteria to identify the beginning of a flare. However, the mean number of flares observed was in line with previously published studies. Nevertheless, information regarding flare duration and organ flaring was not collected.
In conclusion, the LUCIE study provides a reliable insight into SLE clinical profiles and costs of care management in Europe. It showed that the costs are related to disease severity and disease flares, and suggests focusing on preventing flare occurrence and limiting disease progression in order to reduce related costs. The cost of treating SLE patients observed in our study and others is lower than that of other chronic diseases, for example, the cost of multiple sclerosis is 2.5 to 5-times higher to that of SLE;29 however, it appears to be high if we consider the cost/year over a patient's lifetime, especially for severe patients.
SLE care management has improved during the last few years, resulting in a significant increase in patient survival.30 But even if treatment results in long periods of disease remission, SLE remains alternatively active in a high percentage of cases over time.31 Thus other new therapies are needed, to stop disease activity, limit the constant disease evolution and potentially delay the progression of disease.
Acknowledgments
We thank all investigators for their active participation in the study ensuring adequate patient recruitment and allowing a sample close to the target number to be enrolled.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online figure 1
- Data supplement 2 - Online table 1
- Data supplement 3 - Online table 2
- Data supplement 4 - Online table 3
Footnotes
-
Handling editor Tore K Kvien
-
Contributors All authors actively participated in conducting the study, contributed to critical revisions to the manuscript and approved the article for publication. The authors specifically reviewed the manuscript based on their particular field of expertise (eg, clinical, health economics, study design, etc).
-
Funding This study was funded by GlaxoSmithKline, Uxbridge, UK and Human Genome Sciences, Inc, Rockville, Maryland, USA; grant number: study GHO-09-2521, etrack number: BEL114431.
-
Competing interests The Scientific Committee, composed of clinical (AD, ZA, RC, MK, MS and JR), epidemiological (FG) and medico-economic (GK) experts, has received payment for board membership and consultancy from GlaxoSmithKline and Human Genome Sciences. AD has received payment for lectures from GlaxoSmithKline and UCB. ZA was invited to the EULAR 2012 and ACR 2011 congresses. RC has received payment for lectures and educational presentations from GlaxoSmithKline and for board membership from Roche, MedImmune and UCB. MK has received payment for lectures from GlaxoSmithKline/Human Genome Sciences and was invited to the Lupus Academy 2012. MS has received payment for lectures from GlaxoSmithKline. GK has received payment for consultancy and lectures from various pharmaceutical companies. AP, MM and IB are employed by GlaxoSmithKline. CS is employed by and owns stock in GlaxoSmithKline. FM and AG are employed by IMS Health consulting services.
-
Ethics approval According to the local requirements, the study was approved by ethics committees (in Italy, Germany and the UK) and by the regulatory authorities in France and Spain. In Italy, the study was submitted to: the Comitato Etico per la sperimentazione dell'Azienda Ospedaliera di Padova regione Veneto (Padua), the Comitato Etico dell'Azienda Ospedaliera di Farmacologia clinica di Cagliari (Cagliari), the Comitato Etico Locale dell'Azienda Ospedaliera Universitaria Senese, C/o UOC di Farmacia (Siena) and the Comitato Etico dell'Azienda Ospedaliera Universitaria, Seconda Università degli Studi di Napoli (Naples). In Germany, the study was submitted to: the Ethikkommission der Landesärztekammer Rheinland-Pfalz (Bad Kreuznach), the Ethikkommission der Medizinischen Hochschule Hannover (Hanover), the Ethikkommission—Ethikausschuss 1 am Campus Charité—Mitte (Berlin) and the Ethikkommission der Medizinischen Fakultät der HHU Düsseldorf (Düsseldorf) for the principal investigator. The office-based physician participation was approved by the principal investigator ethics committee. In the UK, the study was submitted to: the Joint Clinical Trials Office in London (for the Rayne Institute centre), the Joint UCLH/UCL/Royal Free Biomedical Research (R&D) Unit in London (for St Thomas’ Hospital centre), the Birmingham Clinical Research Office (for the University Hospital Birmingham centre) and the Central Manchester University Hospitals: the Manchester Royal Infirmary Research & Development Office (for the University College London Hospitals). The study was also submitted for (local) R&D approval through the NHS/HSC Research and Development offices.
-
Provenance and peer review Not commissioned; externally peer reviewed.