Article Text

Abstract
Objective To develop recommendations for cardiovascular risk (CVR) management in gout, vasculitis, systemic sclerosis (SSc), myositis, mixed connective tissue disease (MCTD), Sjögren’s syndrome (SS), systemic lupus erythematosus (SLE) and antiphospholipid syndrome (APS).
Methods Following European League against Rheumatism (EULAR) standardised procedures, a multidisciplinary task force formulated recommendations for CVR prediction and management based on systematic literature reviews and expert opinion.
Results Four overarching principles emphasising the need of regular screening and management of modifiable CVR factors and patient education were endorsed. Nineteen recommendations (eleven for gout, vasculitis, SSc, MCTD, myositis, SS; eight for SLE, APS) were developed covering three topics: (1) CVR prediction tools; (2) interventions on traditional CVR factors and (3) interventions on disease-related CVR factors. Several statements relied on expert opinion because high-quality evidence was lacking. Use of generic CVR prediction tools is recommended due to lack of validated rheumatic diseases-specific tools. Diuretics should be avoided in gout and beta-blockers in SSc, and a blood pressure target <130/80 mm Hg should be considered in SLE. Lipid management should follow general population guidelines, and antiplatelet use in SLE, APS and large-vessel vasculitis should follow prior EULAR recommendations. A serum uric acid level <0.36 mmol/L (<6 mg/dL) in gout, and disease activity control and glucocorticoid dose minimisation in SLE and vasculitis, are recommended. Hydroxychloroquine is recommended in SLE because it may also reduce CVR, while no particular immunosuppressive treatment in SLE or urate-lowering therapy in gout has been associated with CVR lowering.
Conclusion These recommendations can guide clinical practice and future research for improving CVR management in rheumatic and musculoskeletal diseases.
- autoimmune diseases
- cardiovascular diseases
- lupus erythematosus
- systemic
- systemic vasculitis
- antiphospholipid syndrome
Statistics from Altmetric.com
- autoimmune diseases
- cardiovascular diseases
- lupus erythematosus
- systemic
- systemic vasculitis
- antiphospholipid syndrome
Introduction
Patients with inflammatory rheumatic diseases have an increased risk of cardiovascular disease,1 in comparison to the general population, which prompted the development (2010) and update (2015/16) of European League against Rheumatism (EULAR) recommendations for cardiovascular risk (CVR) management in patients with rheumatoid arthritis (RA), ankylosing spondylitis and psoriatic arthritis.2 Accumulating evidence has shown elevated cardiovascular morbidity and mortality in other rheumatic and musculoskeletal diseases (RMDs) including gout, vasculitis, systemic sclerosis (SSc), myositis, mixed connective tissue disease (MCTD), Sjögren’s syndrome (SS), systemic lupus erythematosus (SLE) and the antiphospholipid syndrome (APS).3–13 Estimations of the incidence of cardiovascular events vary among the different disease groups (Supplementary systematic literature review (SLR) report, section II).
The higher CVR in patients with rheumatic diseases is not sufficiently explained by differences in the prevalence of traditional CVR factors,14–18 suggesting that specific treatment recommendations tailored to patients with these conditions are needed. Chronic inflammation has been considered a key feature in cardiovascular disease pathogenesis in RMDs,19 demonstrated also in the general population by associations with serum C-reactive protein (CRP) levels20 21 and the efficacy of medications targeting inflammatory pathways,22–24 while new links between inflammation, immunity and cardiometabolic factors are being researched.25 Furthermore, patients with RMDs are often exposed to immunomodulators and glucocorticoids. Although better control of inflammation may reduce CVR in individual patients,23 24 it is not known if some side effects of these medications might outweigh any anti-inflammatory benefit, thereby increasing the CVR.
Therefore, a EULAR Task Force was formed to develop recommendations for the management of CVR in patients with SLE, APS, gout, vasculitis, SSc, myositis, MCTD and SS based on an evidence-based approach and experts’ consensus.
Methods
Task force
Two convenors (MTN and MGT) guided the task force together with two methodologists (GJM and MMW) and four fellows (DV, GCD, EH and LB), responsible for the SLRs. Furthermore, the task force included 20 members from 11 European countries: 12 rheumatologists, 2 cardiologists, 1 metabolic medicine physician, 1 healthcare professional, 2 patient representatives and 2 EMerging EULAR NETwork members (KS and SS). The process followed the updated EULAR standardised operating procedures26 and the Appraisal of Guidelines for Research and Evaluation II instrument.27
At the initial task force meeting, a first set of research questions, prepared by the convenors, was discussed with the panel and formulated on four major topics: use of cardiovascular prediction tools; interventions targeting traditional CVR factors; interventions targeting disease-related CVR factors and prevalence/incidence of cardiovascular disease. Thereafter, final research questions were developed using the PICO format (P, population; I, intervention; C, comparator; O, outcomes).
Collection of evidence
A comprehensive SLR was performed by two groups working in parallel: the gout, vasculitis, SSc/myositis/MCTD/SS group (convenor: MTN; methodologist: GJM; fellows: DV, EH and LB), and the SLE and APS group (convenor: MGT; methodologist: MMW; fellow: GCD). The protocol for the literature search was based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement.28 Search terms were developed with the help of experienced librarians of the VU Αmsterdam, Northwest Clinics Alkmaar (for gout, vasculitis, SSc, myositis, MCTD and SS SLRs) and the National Institutes of Health, USA (for SLE and APS SLRs). PubMed, Embase and the Cochrane Library were searched for full-length English-language published articles from their inception to March 2020, while searches for incidence and prevalence of cardiovascular events were extended up to November 2020. Exclusion criteria and the search terms for each disease separately are presented in the Supplementary SLR report (section IA). The outcome was cardiovascular events rather than surrogate markers of cardiovascular disease.
Data abstraction is described in Supplementary SLR report (section IB). Retrieved studies were screened by title and abstract and articles selected for full text review were then examined independently by two persons for each group (DV, EH, LB, MN, CM, and GCD, MGT and MMW) with consultation of other task force members. A number of individually searched articles (one for gout,29 three for SLE/APS30–32 published after the initial search periods were included due to their importance. Data extraction was performed by the fellows (DV, EH and LB) and CM under supervision of MN and GJM in the gout, vasculitis, SSc, myositis, MCTD and SS group, and by GCD, MGT and MMW in the SLE and APS group. Quality assessment was performed using the Cochrane risk-of-bias tool33 for randomised clinical trials and the Newcastle-Ottawa Scale34 for observational studies. Formal pooling and meta-analysis of risks could not be performed due to the diversity of outcomes, exposures and measures of association reported in the primary studies. Evidence summaries and draft recommendations were formulated for review by all task force members before the second meeting.
Consensus on statements
The virtual second task force meeting included the presentation of SLR results and discussion and editing of the first draft of recommendations. Recommendations were accepted when ≥75% of the task force members voted agreement. After additional discussions on wording changes and voting on text, a final set of recommendations and overarching principles was prepared, including the level of evidence (LoE) and grade of recommendation (GoR) according to the Oxford Centre for Evidence Based Medicine system.35 All task force members indicated their level of agreement (LoA) for each recommendation (0, no agreement at all; 10, full agreement), and results were averaged. The manuscript was reviewed and approved by all task force members and the EULAR Executive Committee before submission.
Results
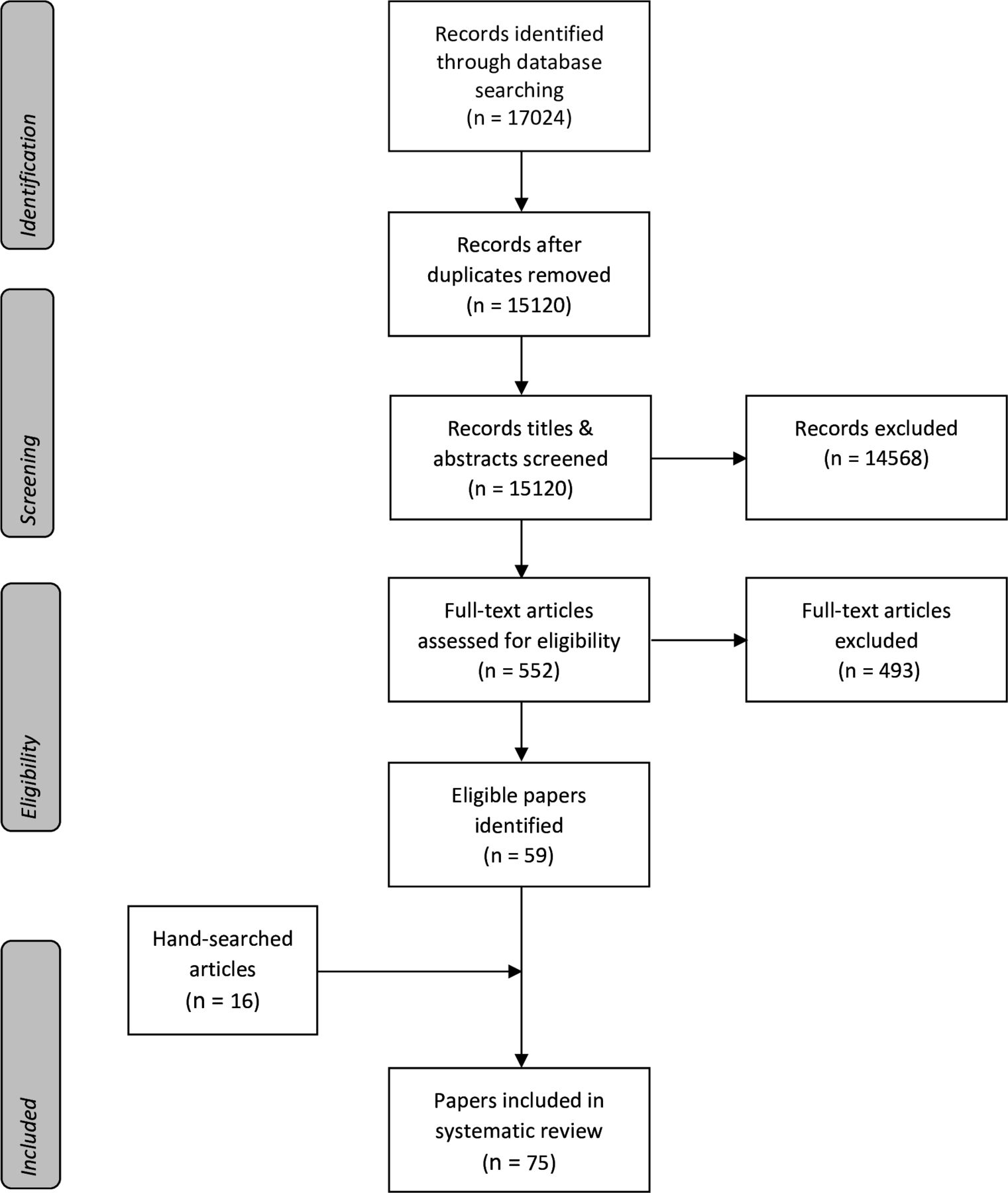
For gout, vasculitis, SSc, myositis, MCTD and SS, 105 articles were included in the SLR, while for SLE and APS, 75 articles were included (figures 1 and 2). SLR results including the flow chart and evidence tables for each PICO are presented in Supplementary SLR report (section II); all articles included in the SLRs are shown in section III.
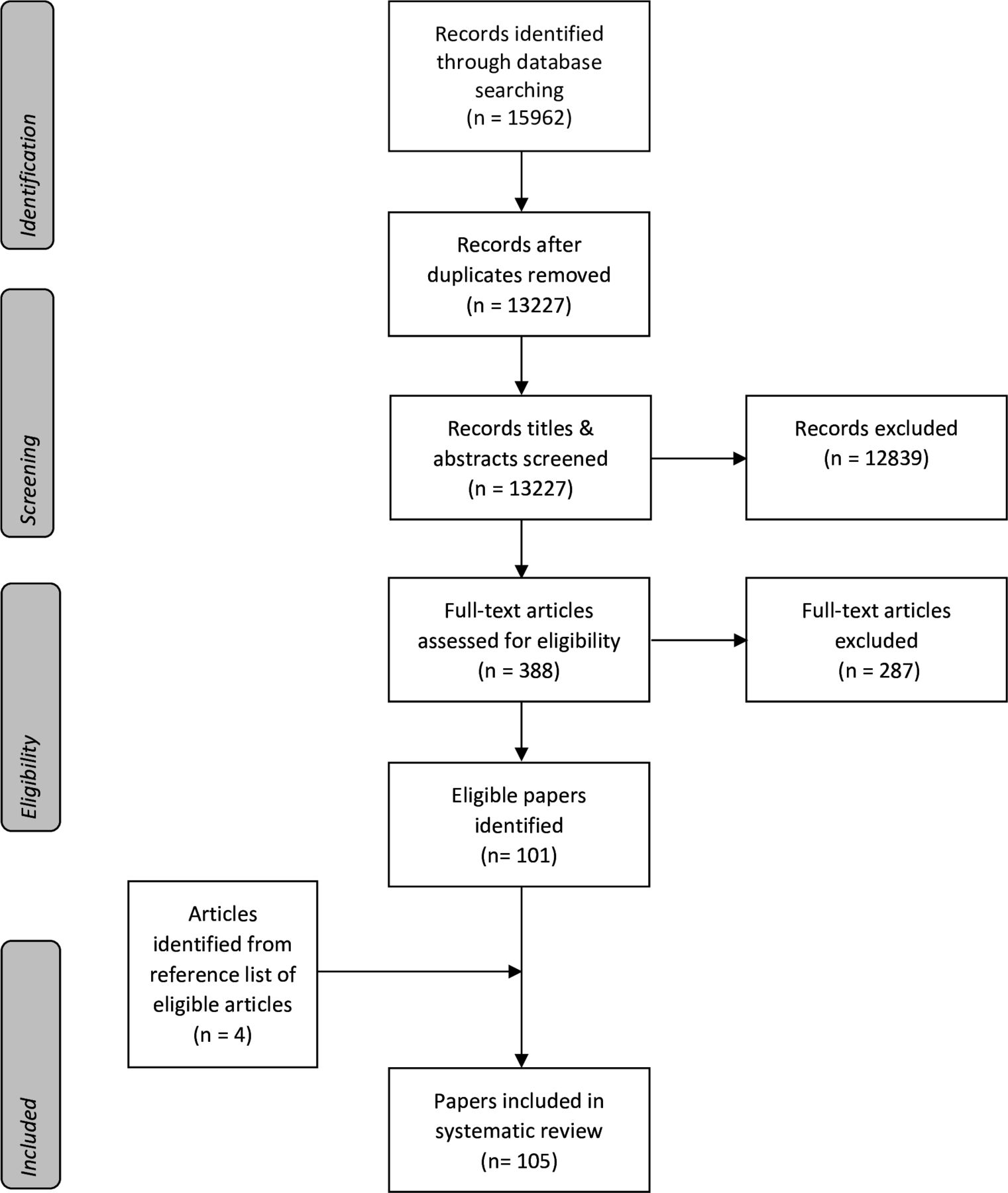
Flow chart of systematic literature review for cardiovascular risk management in gout, vasculitis, systemic sclerosis, myositis, mixed connective tissue disease and Sjögren’s syndrome. Articles on cardiovascular incidence and prevalence are also included.

{kind=link}
{kind=link}
Flow chart of systematic literature review for cardiovascular risk management in systemic lupus erythematosus and the antiphospholipid syndrome.
Overarching principles
The task force developed four overarching principles emphasising the need for increased awareness of elevated CVR in RMDs, regular CVR screening, assessment and management of modifiable CVR factors, and patient education about CVR, treatment adherence and lifestyle changes (table 1).
EULAR overarching principles and recommendations for the management of CVR in gout, vasculitis, SSc, myositis, MCTD, SS, SLE, and APS
Recommendations
Gout, vasculitis, SSc, myositis, MCTD and SS
CVR prediction tools
1. In patients with gout, vasculitis, SSc, myositis, MCTD and SS, we recommend thorough assessment of traditional CVR factors. The use of cardiovascular prediction tools as for the general population is recommended. (LoE: 5, GoR: D)
No studies have investigated the accuracy of cardiovascular prediction tools in patients with gout, vasculitis, SSc, myositis, MCTD and SS. It is currently uncertain to what extent the elevated risk for cardiovascular disease is driven by an increased prevalence of traditional or disease-specific risk factors. Existing tools, such as the Framingham Risk Score (FRS), QRISK3 or Systematic Coronary Risk Evaluation (SCORE) have been based on large general population cohorts with long follow-ups.36–38 Therefore, for gout, vasculitis, SSc, myositis, MCTD and SS, we recommend the use of prediction tools developed in the general population.
2. For ANCA-associated vasculitis the Framingham score may underestimate the CVR. Information from the European Vasculitis Society (EUVAS) model may supplement modifiable Framingham risk factors and is recommended to take into account. (LoE: 2b, GoR: D)
In patients with ANCA-associated vasculitis the observed incidence of cardiovascular events exceeded Framingham predicted incidence in two studies.39 40 Furthermore, one study on CVR in ANCA-associated vasculitis found a higher area under the curve (AUC) for the EUVAS model (AUC 0.73) based on age, diastolic hypertension, and PR3 ANCA status in comparison with the Framingham model (AUC 0.65).41 Although this study was not designed for the evaluation of CVR, these disease-specific factors could be used for risk assessment in addition to Framingham risk factors but further work is needed to validate these findings.
Interventions targeting traditional CVR factors
3. In patients with gout, vasculitis, SSc, myositis, MCTD, and SS, blood pressure (BP) management should follow recommendations used in the general population. (LoE: 5, GoR: D)
We found no trials that assessed the use of antihypertensive treatment in these patients. One small retrospective cohort study found an increase of severe cranial ischaemic events in patients with giant-cell arteritis (GCA) treated with beta blockers.42 One large prospective cohort study in SSc found a protective effect of calcium channel blockers (CCB), ACE inhibitors (ACEI), and angiotensin receptor blockers (ARB) with ventricular arrhythmias.43 Both studies did not control for confounding by indication. Altogether, currently, there is no evidence to modify the hypertension treatment target levels in patients with gout, vasculitis, SSc, myositis, MCTD and SS from those used in the general population.
4. In patients with gout, diuretics should be avoided. (LoE: 5, GoR: D)
Following the EULAR recommendations on management of gout, use of thiazide and loop diuretics should be avoided, if possible, because of their effect to increase serum uric acid (SUA) levels.44 Instead, the use of CCB or losartan could be considered. This topic was not updated as part of this guideline as the literature search focused on the effect of antihypertensives on cardiovascular outcomes and not on potential effect on SUA levels.
5. In patients with SSc beta blockers should be avoided. (LoE: 5, GoR: D)
Although large trials are lacking and therefore based on expert opinion, beta blockers are considered contraindicated due to their effect on Raynaud’s phenomenon.
6. In patients with gout, vasculitis, SSc, myositis, MCTD, and SS, lipid management should follow recommendations used in the general population. (LoE: 5, GoR: D)
In gout patients, no studies evaluated the effect of statins on cardiovascular disease or mortality in comparison with the general population. Two retrospective cohort studies suggested a protective effect of statins on mortality in patients with gout after 5 and 10 years, relative to patients not using statins.45 46 Because of the limited evidence, we recommend following guidelines on lipid management for the general population. Furthermore, myotoxicity as side effect of the combination of a statin and prophylactic colchicine (0.5 mg/day) is rare and routine discontinuation of the statin is not recommended.47
Three studies in patients with GCA did not find an association between statins and cardiovascular events,42 48 49 but a fourth study of 103 patients with GCA, 28 of whom were treated with statins, reported a lower risk of cardiovascular hospitalisations with a longer cumulative duration of statin treatment (HR 0.993 per one additional daily dose).50 No studies controlled for confounding by indication.
7. In patients with gout, vasculitis, SSc, myositis, MCTD, and SS, standard use of low-dose aspirin for primary prevention is not recommended. Treatment with platelet inhibitors should follow recommendations used in the general population. (LoE: 2b/5, GoR: D)
In 2009 EULAR recommended the use of aspirin for prevention of cardiovascular and cerebrovascular events in individuals with large vessel vasculitis (LoE: 3, GoR: C).51 More recently the American College of Rheumatology (ACR) has used the same literature base to conditionally recommend the use of aspirin in flow critical large vessel vasculitis.52 However, in 2020 an update of the 2009 EULAR recommendations reappraised this evidence and concluded that the risk–benefit analysis was not favourable, and blanket use of antiplatelets was not essential unless indicated for other reasons.53 Based on newly published studies, we agree with the 2020 iteration.41 48 49 In patients with gout, ANCA-associated vasculitis, SSc, myositis, MCTD and SS we did not find studies on this topic.
8. In patients with gout, we recommend a SUA level below 0.36 mmol/L (6 mg/dL) to potentially lower the risk of cardiovascular events and cardiovascular mortality. (LoE: 2b, GoR: C)
Retrospective cohort studies in patients with gout showed an association between an elevated SUA (per 0.06 mmol/L (1 mg/dL)) and cardiovascular events.54 55 The association might be stronger in patients with SUA levels above 0.48 mmol/L (8 mg/dL),56 than in patients with SUA levels higher than 0.36 mmol/L (6 mg/dL).57 Studies on the effect of urate-lowering therapy (ULT) showed conflicting results. Evidence originates predominantly from observational studies and often lacked data on treatment adherence and SUA levels during treatment. One study showed a linear dose response relation with a decline in the CVR in the group with the highest defined daily dose.58 This suggests that adequate ULT possibly lowers the CVR. This possibility was supported by two studies that showed a protective association of respectively ‘high dose’ allopurinol and ULT resulting in SUA <0.36 mmol/L (<6 mg/dL) on cardiovascular events and cardiovascular mortality.59 60 Altogether, although numbers of events were often low and associations were stronger for the highest SUA quartiles and higher dose ULT, it is possible that achieving lower SUA level decreases the risk on CV events. A cut-off value of 0.36 mmol/L (6 mg/dL) is used in the management of gout activity and could also benefit the risk of cardiovascular events. There is not sufficient evidence to support a threshold lower than 0.36 mmol/L (6 mg/dL) for CVR management.
9. In patients with gout there is no preference for a particular ULT from the cardiovascular point of view. (LoE: 1b, GoR: B)
Current guidelines recommend allopurinol as the first choice of ULT followed by febuxostat. Most studies on CVR compared these two xanthine oxidase inhibitors. Overall, regardless of the used dosage and duration of treatment, no difference was seen in number of cardiovascular events.61–63 In 2018, the CARES trial reported a higher risk of cardiovascular mortality with febuxostat than allopurinol.62 However, no difference was seen in the primary composite cardiovascular disease endpoint. Recently, the FAST trial showed no difference in CVR between patients using allopurinol or febuxostat.29 Because of the limitations of the CARES trial (high number drop-outs, no difference in primary outcome, most events occurred after discontinuation of study) and the non-inferiority results of the FAST trial, we do not recommend the use of a specific ULT regarding cardiovascular outcomes.
Interventions targeting disease-related CVR factors
10. In patients with ANCA-associated vasculitis, remission induction and remission maintenance will also reduce CVR. (LoE: 2b, GoR: D)
In three of four included studies an association was found between high disease activity scores (Birmingham Vasculitis Activity Scores version 3) and a higher risk for cardiovascular events.64–66
11. In patients with GCA an optimal glucocorticoid regimen that balances the risk of relapse and glucocorticoid use side effects may be considered to also reduce CVR. (LoE: 2b, GoR: D)
In patients with vasculitis, SSc, myositis, MCTD, and SS the primary goal is disease control with the lowest possible dose of glucocorticoids. In GCA two studies found a higher CVR in patients with a higher (daily/cumulative) prednisone dose. One study found that the use of an immunosuppressant in addition to glucocorticoid was a protective factor against new cardiovascular events.67 68 The increased CVR associated with glucocorticoids has to be balanced with the risk of relapse. Special attention and frequent evaluation of risks and benefits are warranted for patients with ongoing low dose glucocorticoids.
SLE and/or APS
CVR prediction tools
1. In patients with SLE and/or APS, a thorough assessment of traditional CVR factors and disease-related risk factors is recommended to guide risk factor modification. (LoE: 2b, GoR: D)
The FRS underestimates CVR in SLE patients18 69–71 with stroke, more often than myocardial infarction (MI), accounting for excess ‘missed’ risk by the FRS.69 70 A modified version of the FRS that used a 2.0 multiplier was found, retrospectively, to improve the measure’s sensitivity from 0.13 to 0.31 while maintaining good specificity to identify patients with a moderate/high risk of coronary artery disease.72 A study examining cardiovascular mortality in middle-aged patients with SLE found that SCORE predicted less than half the observed fatal cardiovascular events.73 The QRISK3 tool included weights for SLE,38 but validation studies in SLE populations have not yet been performed. Direct comparison of the performance of most commonly used generic risk assessment tools in SLE is currently lacking. A new SLE-specific risk score that included disease-related variables (SLEDAI, lupus anticoagulant and low C3) along with traditional risk factors found higher estimated risks than the American College of Cardiology/American Heart Association risk equation, except among patients whose risk was already moderate/high from traditional risk factors.74 This prediction equation requires more testing and independent validation. Given the limitations of the current evidence, the task force did not endorse use of any particular CVR assessment tool, but instead recommended a thorough assessment of traditional and disease-related risk factors to guide cardiovascular prevention interventions.
No studies were identified that examined generic CVR prediction scores in APS. The adjusted Global APS Score (aGAPSS), a clinical score including the three major antiphospholipid antibodies (aPL), hypertension and lipidaemia, was developed to predict thrombosis, though data on cardiovascular events were not reported separately.75 Modification of the aGAPSS by adding points for diabetes mellitus, smoking, and obesity to create a score specific for cardiovascular disease, the aGAPSSCVD score, increased its discriminative ability and accuracy for CVR prediction in one study,76 but further testing is needed.
Interventions targeting traditional CVR factors
2A. In patients with SLE, lower levels of BP are associated with lower rates of cardiovascular events and a BP target of <130/80 mm Hg should be considered. (LoE: 2b, GoR: C)
2B. In patients with lupus nephritis, ACEi or ARBs are recommended for all patients with urine protein-to-creatinine ratio >500 mg/g or arterial hypertension. (LoE: 5, GoR: D)
2C. In patients with APS, hypertension management should follow recommendations used in the general population. (LoE: 5, GoR: D)
A. SLE. Hypertension is associated with a higher risk of both coronary artery disease events77 and first ischaemic stroke78 in SLE. It, therefore, follows that BP control with antihypertensive medications should reduce the risk of cardiovascular events.79 Recent mean systolic BP ≥132 mm Hg was identified as a determinant of a higher risk of cardiovascular events, and systolic BP had a stronger association than diastolic BP.80 A recent study of patients with SLE examining three BP categories (normotensive; systolic BP 130–139/diastolic BP 80–89; systolic BP ≥140/diastolic BP ≥90 mm Hg) reported an increased risk of cardiovascular events in both hypertensive groups compared with the normotensive group,30 suggesting that a target BP of less than 130/80 should be used.
B. Lupus nephritis. Evidence specifically addressing the impact of antihypertensive treatment on cardiovascular events in lupus nephritis is scarce. In a retrospective cohort analysis,81 risk of a cardiovascular event was not associated with treatment with ACEI/ARB, but 18% in the ACEI/ARB group had end-stage renal disease compared with 2.4% in the comparison group and this imbalance would be expected to affect the comparison of CVRs. The panel endorsed the current EULAR/ERA-EDTA recommendation on the use of ACEI/ARB for patients with lupus nephritis with concomitant hypertension or high-level proteinuria.32
C. APS. No studies were identified on the use of specific antihypertensives for cardiovascular prevention in patients with APS. These patients should be managed according to recommendations for the general population.82
3. In patients with SLE and/or APS, hyperlipidaemia treatment should follow recommendations used in the general population. (LoE: 5, GoR: D)
Higher levels of total cholesterol and low-density lipoprotein cholesterol have been associated with a higher risk of MI and stroke in SLE.74 78 83 One study using national administrative data found that patients with SLE treated with lipid-lowering agents had a significantly lower risk of coronary artery disease during follow-up (mean 8.4 years) than those not treated, while short-duration or long-duration statin use were both associated with a lower risk of stroke.84 Several other observational studies included statin use as a covariate in prediction of cardiovascular events, and identified statin use as a risk factor for events, likely representing confounding by indication.71 85–88 Diagnosis of SLE is not sufficient per se for prescribing lipid-lowering treatment for primary cardiovascular prevention.89 In APS, no study was identified that examined the effect of lipid-lowering agents on cardiovascular events. The task force judged that hyperlipidaemia treatment should follow the recommendations used in the general population.89
4A. Patients with SLE may be candidates for preventive strategies as in the general population, including low-dose aspirin, based on their individual CVR profile. (LoE: 2b, GoR: D)
4B. In asymptomatic aPL carriers with a high-risk profile with or without traditional risk factors, prophylactic treatment with low-dose aspirin (75–100 mg daily) is recommended. (LoE: 2 a, GoR: B) In patients with SLE and no history of thrombosis or pregnancy complications, prophylactic treatment with low-dose aspirin is recommended for those with a high-risk aPL profile (LoE: 2a, GoR: B) and may be considered for those with a low risk APL profile. (LoE: 2b; GoR: C)
The panel agreed to include the corresponding statements (and LoE and GoR) about the prophylactic use of antiplatelets in SLE and APS from the recent EULAR recommendations for the management of SLE90 and APS,91 respectively. The LoA from our task force group is shown in table 1. Use of low-dose aspirin for cardiovascular prevention in patients with SLE or APS should be individualised (particularly in the presence of a high-risk aPL profile) according to EULAR recommendations.
Interventions targeting disease-related CVR factors
5. In patients with SLE, low disease activity should be maintained to also reduce CVR. (LoE: 2b, GoR: B)
SLE activity has often been reported as a predictor of cardiovascular events. With the exception of two studies,86 92 higher time-integrated SLEDAI levels were associated with an increased risk of cardiovascular events,69 77 79 93 more so than baseline or single measurements.78 94 95 In three studies,71 96 97 baseline SLEDAI was found to be higher in patients with cardiovascular events, although it was not carried to multivariable analysis. Associations of SLEDAI with cardiovascular events was found to be stronger when considering categories of activity compared with per-unit increases,69 suggesting a non-linear association of disease activity with cardiovascular events.
Many studies did not consider simultaneously the association of measures of disease activity and SLE medication use; therefore, results may be confounded. In an analysis that adjusted for current prednisone dose, a 1-point increase in SLEDAI was marginally associated with an increased risk of cardiovascular events (relative risk 1.05, 95% CI 1.00 to 1.11).69 Available evidence indicates that higher disease activity may be associated with a higher risk of cardiovascular events. Thus, in addition to its importance in general patient management,90 a low-disease activity state may also have a beneficial effect on cardiovascular health.
6. In patients with SLE, treatment with the lowest possible glucocorticoid dose is recommended to minimise any potential cardiovascular harm. (LoE: 2b, GoR: C)
Mean dosage, cumulative exposure and duration of glucocorticoid treatment have all been investigated with reference to cardiovascular events in SLE. Higher current glucocorticoid dose was associated with a higher risk of atherothrombotic events, ischaemic heart disease, and/or stroke in two studies,69 98 but was protective in one study79 and not associated with stroke in the SLICC inception cohort.99 Higher mean daily doses, greater cumulative doses, and ever-use of prednisone 30 mg/day or more were more consistently associated with increased risks of cardiovascular events in both cohort and case-control studies,71 92 100 101 although glucocorticoid use was not significantly associated with cardiovascular events in two analyses of the Toronto cohort.95 97 Not all studies adjusted for SLE activity. A retrospective study that adjusted for SLE activity98 found that higher daily doses (prednisone >10 mg) administered continuously were significantly associated with both MI and stroke. In a retrospective and non-randomised study, patients treated at clinics following a glucocorticoid dose-minimisation strategy had lower prednisone exposures and markedly lower risks of cardiovascular damage by the SLICC measure, particularly for stroke.102 Most evidence suggests that higher glucocorticoid exposure (cumulative and mean daily dose) increases CVR in SLE. The task force recommended treatment with the lowest possible corticosteroid dose to minimise risks of cardiovascular harm.
7. In patients with SLE, no specific immunosuppressive medication can be recommended for the purpose of lowering the risk of cardiovascular events. (LoE: 2b, GoR: C)
Use of immunosuppressants as a class in SLE have had largely null or conflicting associations with cardiovascular events.79 99 103 Three studies from the Toronto lupus cohort reported either a protective96 or null association,93 97 while one study found that patients treated with immunosuppressants vs those not treated were more likely to develop a cardiovascular event in univariate but not multivariate analyses.95 Immunosuppressive therapy was also associated to higher odds of ischaemic heart disease and cardiovascular events in the LUMINA104 and Hopkins lupus cohort.69
Studies of individual medications suggest that use of methotrexate, mycophenolate, cyclosporine, or rituximab had neutral associations with cardiovascular events.88 92 105 Conflicting results have been reported for cyclophosphamide71 106 and azathioprine.71 88 106
A common limitation in many studies was the examination of ever use vs never use of immunosuppressants, which may be too crude an exposure. No studies considered issues of confounding by indication, and positive associations with cardiovascular disease may reflect risks due to associated disease activity or severity, or concomitant glucocorticoid use. Based on current evidence, the task force concluded that no specific immunosuppressive medication can be recommended for reducing the risk of cardiovascular events. Furthermore, the committee call for better quality pharmacoepidemiologic studies in future, using recent advances in this field.
8. In patients with SLE, treatment with hydroxychloroquine (which is recommended for all SLE patients, unless contraindicated) should be considered to also reduce the risk of cardiovascular events. (LoE: 2b, GoR: B)
A large body of evidence has addressed the role of antimalarials in cardiovascular prevention in SLE. In six cohort studies, antimalarial use was associated with lower risk of either atherothrombotic events or coronary artery disease,69 77 79 88 94 107 although in one study protection was only associated with current long-term use.69 Several other studies reported null associations.85 87 92 93 95 103 106 Two of seven case–control studies also reported less use of hydroxychloroquine or antimalarials among cases with cardiovascular events than controls,100 108 with only one study reporting increased risk.97 No associations with risk of stroke specifically have been reported.99 109 Importantly, patients with less active disease are more often treated with antimalarials, while SLE activity may be the risk factor for cardiovascular disease; this possible selection bias was not addressed. Additionally, studies did not report results stratified by the presence of APS or aPL, therefore, it is unclear if any reduced risk is limited to patients with SLE and aPL. The task force endorsed treatment with hydroxychloroquine, as should be provided to all patients with SLE, as it may also reduce the risk of cardiovascular events.
Discussion
The 2021 EULAR recommendations for CVR management in RMDs comprise overarching principles and guidance informed by the currently available evidence on several potential interventions aiming to improve cardiovascular outcomes in these disorders. The LoA for most statements was high, indicating a coherent perspective on behalf of health professionals from different areas of care and patients alike for CVR reduction efforts.
The majority of the included RMDs are uncommon diseases limiting the ability to perform large observational studies to assess the impact of traditional and disease-specific risk factors on cardiovascular disease burden and clinical trials on the long-term cardiovascular effects of preventive treatments. One of the main challenges of these recommendations was the low LoE due to few studies on many of the research questions. Confounding by indication and lack of propensity adjustment was a common limitation in the included studies and therefore several statements relied on expert opinion. Future studies that better identify exposures and outcomes may help overcome these methodological issues.
There are several additional issues that need to be addressed in the future efforts for CVR management in RMDs. Systemic RMDs are complex diseases with a wide range of clinical manifestations of various severity that may affect cardiovascular health in diverse ways. Considering personalised patient care, the potential impact of individual patient clinical phenotype on cardiovascular prognosis also merits further investigation. In guidelines for cardiovascular prevention in the general population, risk stratification represents a prerequisite for CVR management (eg, BP targets or lipid-lowering therapy).82 89 In this context, it is important to recognise that underperformance of clinical CVR prediction tools used in the general population may hamper CVR prevention and management in RMDs. The use of prediction tools that incorporate CRP110 (eg, Reynolds risk score111), the presence of specific RMDs (RA, SLE) or anti-inflammatory agents (eg, QRISK3)38 or multipliers of baseline risk (eg, modified SCORE)112 has been suggested by some guideline committees for CVR stratification in the general population but their use in RMDs needs to be further tested and validated. Thus, studies on disease-specific tools for CVR assessment including disease-specific in addition to traditional CVR factors, as well as risk qualifiers including the evaluation of the predictive value of nonclinical tools, are warranted. These issues, along with other relevant questions such as the pragmatic use of any risk score (simplicity often aids use) will hopefully inspire future research increasing the quality of evidence in CVR management in RMDs, are presented in the Research Agenda (box 1). One of future challenges is the better identification of patient subgroups at higher CVR including for example those with longer disease duration, and number of flares/relapses (eg, in SLE, vasculitis, gout)55 66 113–115 or those with certain demographic (age, gender, race/ethnicity)116 and disease characteristics (eg, aPL positivity in SLE, polyarticular or tophaceous phenotype in gout).55 113 117
Research agenda and future perspectives
Validation of existing generic and modified CVR prediction tools in large prospective studies, and development of new disease-specific equations.
Additive value of vascular imaging and/or circulating biomarkers in CVR assessment in RMDs.
Identification of patient subgroups with higher CVR.
Long-term effects of current and new drugs for RMDs on CVR factors and cardiovascular events.
Role of antithrombotic agents used in some RMDs (eg, aspirin, LMWH in SLE/APS) to reduce the overall CVR in these patients.
Need for large educational campaigns within the rheumatological and other medical specialties and patient associations to increase CVR awareness.
Best implementation methods for the CVR recommendations.
APS, antiphospholipid syndrome; CVR, cardiovascular risk; LMWH, low-molecular weight heparin; RMDs, rheumatic and musculoskeletal diseases; SLE, systemic lupus erythematosus.
Long-term effects of current and new drugs for RMDs on CVR need further investigation. The deleterious cardiometabolic effects of the excessive exposure to glucocorticoids are well known.118 Current recommendations by the ACR119 and the EULAR53 90 120 121 for the management of RMDs emphasise the adverse effects and the need of the limited dose of glucocorticoids. Limiting glucocorticoid exposure to the lowest effective dose to control active disease for the shortest duration possible and eventually discontinuation, as well as weighting the benefits and risks before starting systemic glucocorticoids, can help reduce cardiovascular harm. Several anti-inflammatory agents (eg, colchicine,122 anti-IL1b123) have been shown to lower cardiovascular outcomes in randomised controlled trials for secondary prevention of cardiovascular disease in the general population and other trials are ongoing (eg, hydroxychloroquine124) but further evidence is needed on the cardiovascular outcomes and safety of such immunoregulatory agents in RMDs. Although the role of hydroxychloroquine in APS, and of non-steroidal anti-inflammatory drugs (NSAIDs) in SLE, was examined in our SLR (Supplementary SLR report, section II), the panel agreed that any statement on the use of these medications should be deferred until more robust evidence is available. More evidence is needed about the effect of glucocorticoids, NSAIDs and IL-1 antagonists, the dosage and duration of colchicine treatment, and the risk and benefits of the concomitant use of colchicine and statins in patients with gout.
Most of the recommendations of established low-cost clinical interventions may apply to both high-resource and low-resource countries worldwide. Implementation strategies for promoting CVR management in RMDs include interactive educational workshops involving health professionals, patients and stakeholders with the support of healthcare professional societies and patient associations, social media dissemination and strategies customised to local and national policies such as academic detailing, audits and feedback techniques.
The panel believes that these recommendations will enable healthcare providers and patients to mutually engage in a long-term care pathway tailored to patients’ needs and expectations for improving cardiovascular health in RMDs. As new data accumulate, this first set of ‘best available’ evidence on cardiovascular prevention in gout, vasculitis, SSc, myositis, MCTD, SS, SLE and APS will be timely updated.
Supplemental material
Ethics statements
Patient consent for publication
Acknowledgments
The committee wishes to acknowledge the support of the EULAR Standing Committee on Clinical Affairs and the EULAR Secretariat.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Lay summary
Disclaimer : This is a summary of a scientific article written by a medical professional (“the Original Article”). The Summary is written to assist non medically trained readers to understand general points of the Original Article. It is supplied “as is” without any warranty. You should note that the Original Article (and Summary) may not be fully relevant nor accurate as medical science is constantly changing and errors can occur. It is therefore very important that readers not rely on the content in the Summary and consult their medical professionals for all aspects of their health care and only rely on the Summary if directed to do so by their medical professional. Please view our full Website Terms and Conditions.
Copyright © 2022 BMJ Publishing Group Ltd & European League Against Rheumatism. Medical professionals may print copies for their and their patients and students non commercial use. Other individuals may print a single copy for their personal, non commercial use. For other uses please contact our Rights and Licensing Team.
Footnotes
GCD, DV and EH are joint first authors.
MTN and MGT are joint senior authors.
Handling editor Josef S Smolen
Twitter @cmukhtyar, @UAberdeenEpi, @mariatektonidou
GCD, DV and EH contributed equally.
MTN and MGT contributed equally.
Contributors GCD, DV and EH drafted the manuscript. MN and MGT convened and supervised the project and edited the manuscript. GCD, DV, EH and LB performed the systematic literature review under the supervision of the methodologists and convenors. GJM and MMW supervised the methodology of the systematic literature review and the Delphi process. All authors contributed with comments and revisions and approved the final version.
Funding This study was funded by European Alliance of Associations for Rheumatology, EULAR. Project number: CLI112.
Competing interests GCD, DV, EH, LB, SB, DTB, NB, GK, FM, CM, MR-C, KS, SS, VPvH, GJM, MMW and MN have nothing to declare. FA: research grants from BMS, Celgene, Novartis and Sandoz and consulting fees from AbbVie, Biogen, BMS, Celgene, Janssen, Lilly, Novartis, Pfizer and Sanofi-Aventis, all unrelated to this manuscript; INB: grant from GSK paid to institution, consulting fees from Astra Zeneca, GSK, Eli lilly, UC, MSD paid to institution, support for attending meetings and/or travel from GSK, participation on a data safety monitoring board/or advisory board from Aurinia, Astra Zeneca and ILTOO paid to institution, all unrelated to this manuscript; MÁG-G: grants/research support from AbbVie, MSD, Jansen and Roche paid to institution and personal consulting fees/participation in company sponsored speakers bureau from AbbVie, Pfizer, Roche, Celgene, MSD, Novartis, SOBI and Sanofi, all unrelated to this manuscript; SJ: grants from BMS paid to institution, personal consulting fees from Astra Zeneca, and personal fees from Danish Medicolegal Council, all unrelated to this manuscript; NS: grants paid to institution from Astrazeneca, Boehringer Ingelheim and Roche Diagnostics, personal consulting fees from Afimmune, Amgen, Astrazeneca, Boehringer Ingelheim, Eli-Lilly, Hanmi Pharamceuticals, MSD, Novartis, Novo Nordisk, Pfizer and Sanofi, all unrelated to this manuscript; ES: grant from Merck and honoraria from Janssen, all unrelated to this manuscript; ZS: research grants from Pfizer paid to institution and personal consulting fees from Pfizer, MSD, Lilly, Novartis, Roche, Gedeon Richter, Boehringer Ingelheim, Abbvie, all unrelated to this manuscript; A-KT: speakers fee from Berlin Chemie Menarini, Novarti and personal fees and non-financial support from AstraZeneca and Grünenthal, all unrelated to this manuscript; AT: consulting fees from Magenta Therapeutics and personal fees from Novartis and Idorsia for participation on a Data Safety Monitoring Board or Advisory Board, all unrelated to this manuscript; AV: personal consulting fees from Astra Zeneca and GS, all unrelated to this manuscript; MGT: research grants from Genesis, GSK, MSD, Pfizer and UCB paid to institution, and personal consulting fees from Genesis, GSK and Novartis, all unrelated to this manuscript.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.