Article Text

Abstract
Objective Neutrophils contribute to the SLE pathogenesis. Neutrophil to lymphocyte ratio (NLR) is reported to correlate with disease activity in SLE. The aim of the study was to evaluate whether NLR reflects underlying immunopathogenic activity in SLE, as well as to determine the contribution of each component of NLR, neutrophil and lymphocyte count.
Methods Data were obtained from a cohort of patients with SLE (n=141) recruited at Lund University, Sweden. NLR levels were compared between patients with SLE and healthy controls (n=79). The relationship between NLR and clinical and immunological markers was examined using Mann-Whitney U test and logistic regression analysis. High NLR was defined as above the 90th percentile of healthy individuals.
Results Patients with SLE had elevated neutrophil count (p=0.04) and reduced lymphocyte count (p<0.0001), resulting in elevated NLR as compared with healthy controls (p<0.0001). Patients with high NLR had more active disease, and were more frequently on prednisone use and immunosuppressive medicines. High NLR was associated with immune complex (IC)-driven disease with presence of antidouble-stranded DNA antibodies (p=0.006), circulating ICs (p=0.02) and type I interferon (IFN) activity (p=0.009). Further, high NLR was associated with neutrophil abnormalities, including enrichment for low-density granulocytes (LDGs) (p=0.001), and increased levels of the serum neutrophil activation marker, calprotectin (p=0.02). Assessing the individual components within NLR, that is, neutrophil and lymphocyte count, high neutrophil count was associated with neutrophil activation markers (p<0.0001), whereas low lymphocyte count was associated with type I IFN activity and elevated numbers of LDGs (p=0.006 and p=0.001, respectively).
Conclusions NLR is elevated in patients with SLE as compared with healthy individuals, and is associated with key immunopathological events, including type I IFN activity and neutrophil activation. Neutrophil and lymphocyte count reflected different aspects of the pathogenesis of SLE. Further studies are needed to determine the causality of the associations.
- systemic lupus erythematosus
- interferon
- autoimmune diseases
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
SLE is a chronic, inflammatory autoimmune disease characterised by involvement of several organ systems, including skin, joints, kidney and nervous system. Although the aetiology of the disease is not fully understood, neutrophils have emerged as key effector cells in the SLE pathogenesis. Initial observations in the 1940s described bone marrow neutrophils engulfing large amounts of antibody-coated nuclear debris (immune complexes; ICs) in patients with SLE, later dubbed the ‘lupus erythematosus (LE) cell’.1 More recently, neutrophils have been described to contribute to the SLE pathogenesis through induction of neutrophil extracellular traps (NETs), a process in which nuclear and cytosolic debris is extruded from dying neutrophils.2 In SLE, NETs are thought to be induced by circulating ICs3 or by low-density granulocytes (LDGs), a neutrophil subset enriched in patients with SLE, which can spontaneously undergo NET formation.4 Once released, NETs expose key intracellular autoantigens, including histones and DNA, as well as induce type I interferon (IFN) production through TLR9 and cGAS activation.5 6 Highlighting their important contribution to SLE pathogenesis, inhibition of NET formation, as shown by us and others, ameliorates lupus-like disease in vivo.5 7 Other than NETs, neutrophils release several danger-associated molecular patterns on activation, including calprotectin (S100A8/A9), as well as B cell activating factor, all of which are elevated in patients with SLE.8 9
Given the pathogenic nature of neutrophils in SLE, neutrophil to lymphocyte ratio (NLR), calculated from the routine complete blood count and differential, has been evaluated as a potential biomarker for disease activity and prognosis. Although NLR levels have been suggested to be associated with disease activity and nephritis in patients with SLE,10 11 the underlying mechanisms accounting for an elevated NLR are not well understood. The aim of the current study was to evaluate whether NLR is associated with underlying immunopathogenic mechanisms in SLE.
Methods
Patients
Patients with SLE (n=141) and healthy individuals (n=79) were recruited at Skane University Hospital, Lund, Sweden from 2010 to 2011. Clinical characteristics have previously been reported by our group12 and are summarised in table 1. Disease activity was assessed by Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K). Blood samples were processed for cell isolation, serum and plasma within 1 hour on blood draw.
Demographic and clinical characteristics of the SLE cohort and healthy individuals
Biomarker assays
Levels of calprotectin (S100A8/A9) were analysed by ELISA according to the manufacturer’s instructions (R&D Systems, Minneapolis, Minnesota, USA). Type I IFN activity was measured using a reporter cell system as described previously.12 Briefly, WISH epithelial cells were cultured with patient serum and analysed for induction of six IFN-regulated genes and three housekeeping genes using the Quantigene Plex 2.0 assay according to the manufacturer’s instructions (Panomics, Fremont, California, USA).
Peripheral blood mononuclear cells (PBMCs) were isolated using Lymphoprep according to the manufacturer’s protocol (Axis-Shield PoC, Oslo, Norway). Within the PBMCs, LDGs were identified as CD14+CD15+CD16++ cells with high forward and side scatter properties using flow cytometry.
Levels of ICs were assessed using IC-FLOW. Briefly, neutrophils were incubated with sera, diluted 1:10 and analysed for cell surface FcγRIIA availability by flow cytometry. In the presence of ICs, FcγRIIA is internalised and no signal is detected by flow cytometry, resulting in an inverse correlation between levels of cell surface FcγRIIA and levels of ICs. As a positive control, heat-aggregated IgG of known concentration was used.
Patient and public involvement
Because this data collection was already complete, patients and the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Statistical analysis
Mann-Whitney U test was used to compare continuous variables between groups. Fisher’s exact test was used for analysis of dichotomised variables. The cut-off for high NLR was defined as 2.73, which was the 90th percentile of healthy individuals. Similarly, lymphopaenia was defined as less than 1.3 million lymphocytes/mL (10th percentile of healthy individuals), and neutrophilia was defined as greater than 4.3 million neutrophils/mL (90th percentile of healthy individuals). Variables not having a Gaussian distribution, for example, calprotectin, ICs, IFN and LDGs, were log2-transformed. Logistic regression analyses were used to estimate the OR for the association of each of the biomarkers to dichotomised NLR (high or low), both with and without controlling for immunosuppressive medications. GraphPad Prism and IBM SPSS V.25 were used for analyses. Results were considered statistically significant at p<0.05.
Results
Patients with SLE have elevated NLR compared with healthy individuals
Patients with SLE had significantly higher levels of neutrophils as compared with healthy individuals (median 3.4 vs 2.8×109/L, p=0.04; figure 1A). In contrast, levels of lymphocytes were reduced (median 1.3 vs 1.7×109/L, p<0.0001; figure 1B), resulting in an overall higher NLR (median 2.34 vs 1.54, p<0.0001; figure 1C). Because low leucocyte count is both a component of our primary predictor (NLR) and the outcome (SLEDAI), we removed the contribution of low leucocyte count to the total SLEDAI score (n=8). Patients with high NLR, defined as above the 90th percentile of healthy individuals (>2.73 NLR), had active disease as defined by SLEDAI >0 more frequently (p=0.04; table 1), had a higher prevalence of antidouble-stranded DNA antibodies (p=0.02; table 1) and were on more immunosuppressive medicines, including prednisone and azathioprine (table 1). Further analyses (data not shown) found that active disease was associated with low lymphocyte count (p=0.04), but not with neutrophilia (p=0.85). As part of a sensitivity analysis, patients on prednisone or other immunosuppressive treatment (n=106) were excluded from the analysis. Patients with SLE with no current immunosuppressive treatment (n=36) still had elevated NLR as compared with healthy individuals (p=0.04; figure 1C). All remaining analyses are done for the full SLE cohort. Patients with SLE also had a higher LDG to lymphocyte ratio (LLR) as compared with healthy individuals (p<0.0001; figure 1D). However, in contrast to prior work, LLR did not associate with SLEDAI in our study (p=0.86; data not shown).
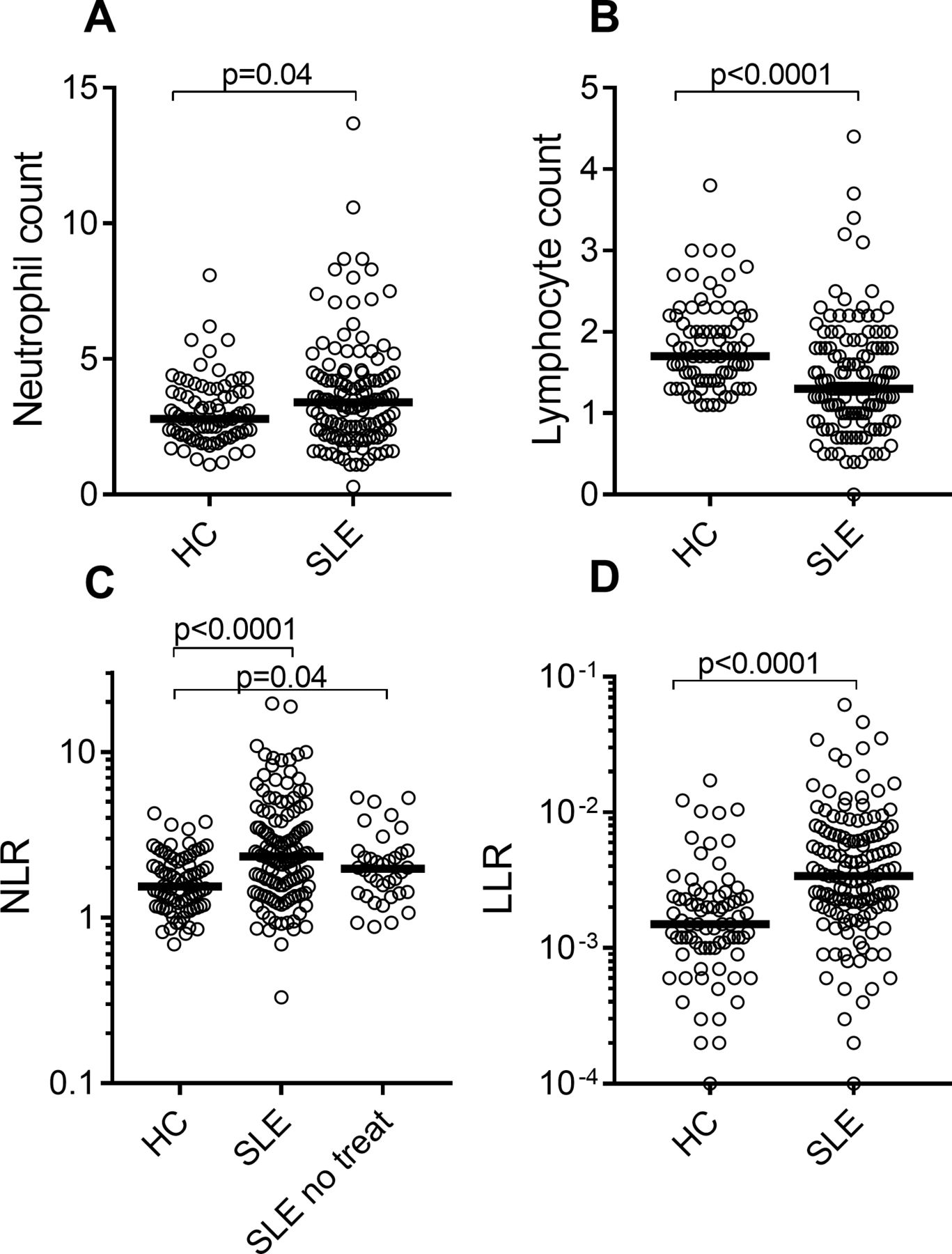
NLR is elevated in SLE and associated with neutrophil activation. Numbers of (A) neutrophils and (B) lymphocytes were assessed in the peripheral blood of HC and patients with SLE. (C) NLR in HC, all patients with SLE and SLE patients without treatment (SLE no treat). (D) LLR in HC and patients with SLE. Statistical analyses were performed using Mann-Whitney U test. HC, healthy controls; LLR, low-density granulocyte to lymphocyte ratio; NLR, neutrophil to lymphocyte ratio.
Elevated NLR is associated with markers of IC-mediated inflammation and neutrophil activation in patients with SLE
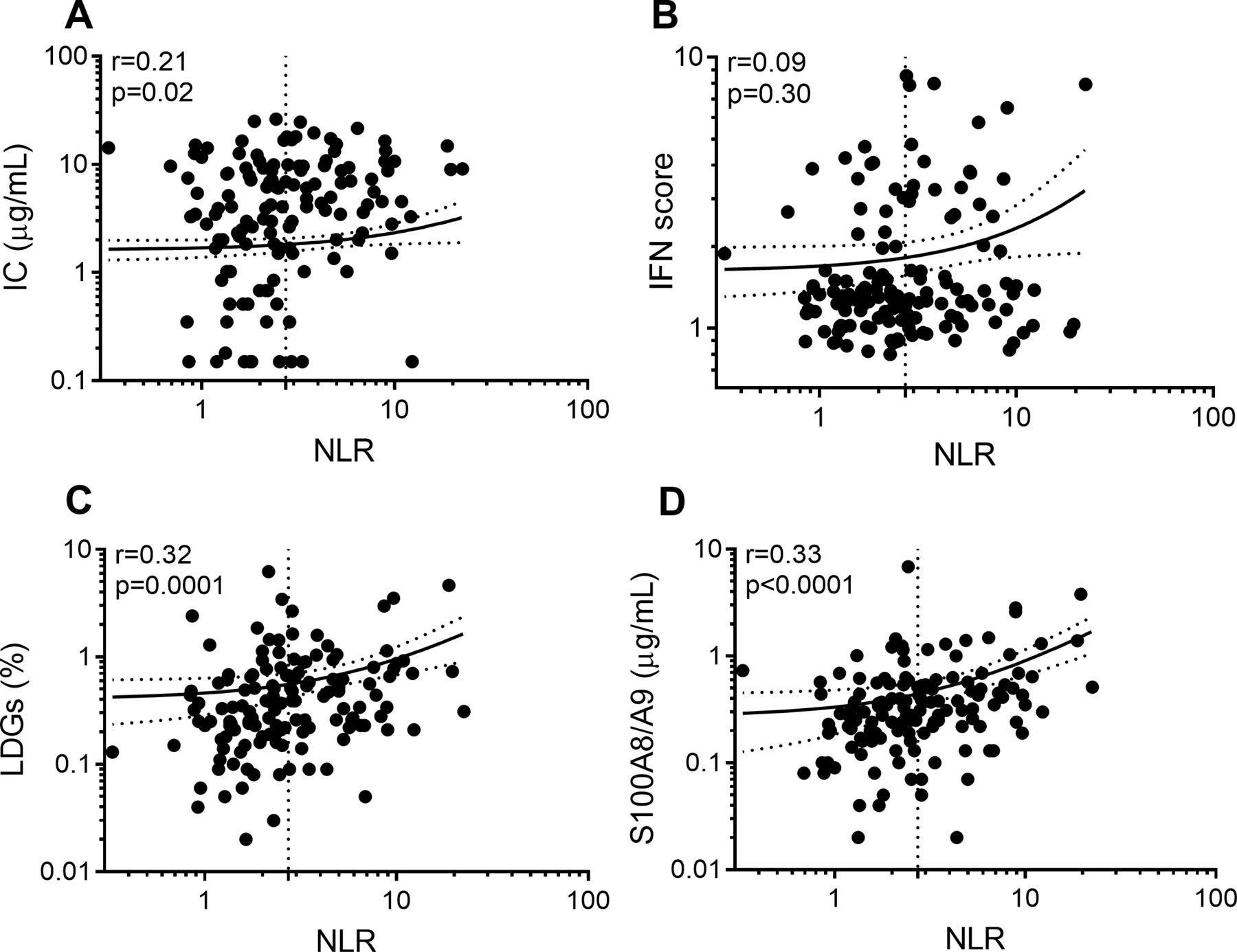
Patients with SLE with high NLR had elevated levels of circulating ICs and type I IFNs when compared with patients with SLE with low NLR (p=0.02 and p=0.009, respectively; figure 2A,B, table 2). Additionally, patients with high NLR had elevated levels of neutrophil activation, as measured by calprotectin (p=0.02; figure 2D, table 2), as well as increased frequency of LDGs (p=0.001; figure 2C, table 2), as compared with patients with SLE with low NLR. These associations were maintained when the models included adjustment for prednisone and immunosuppressive treatment (table 2). Further, levels of NLR correlated with all identified biomarkers except for IFN activity (figure 3). An analysis of the correlations among the biomarkers (data not shown) found that levels of ICs correlated with levels of calprotectin and IFN (r=0.30, p<0.001, and r=0.25, p=0.003, respectively). In addition to NLR, figure 2 also shows the association of neutrophilia and lymphopaenia with the immunological features. Neutrophilia was associated with neutrophil activation marker calprotectin (p<0.0001; figure 2D), which was not seen for lymphopaenia. Further, lymphopaenia was associated with type I IFN activity (p=0.006; figure 2B) and LDG count (p=0.001; figure 2C). Neither of the individual cell count numbers were associated with levels of circulating ICs (figure 2A).
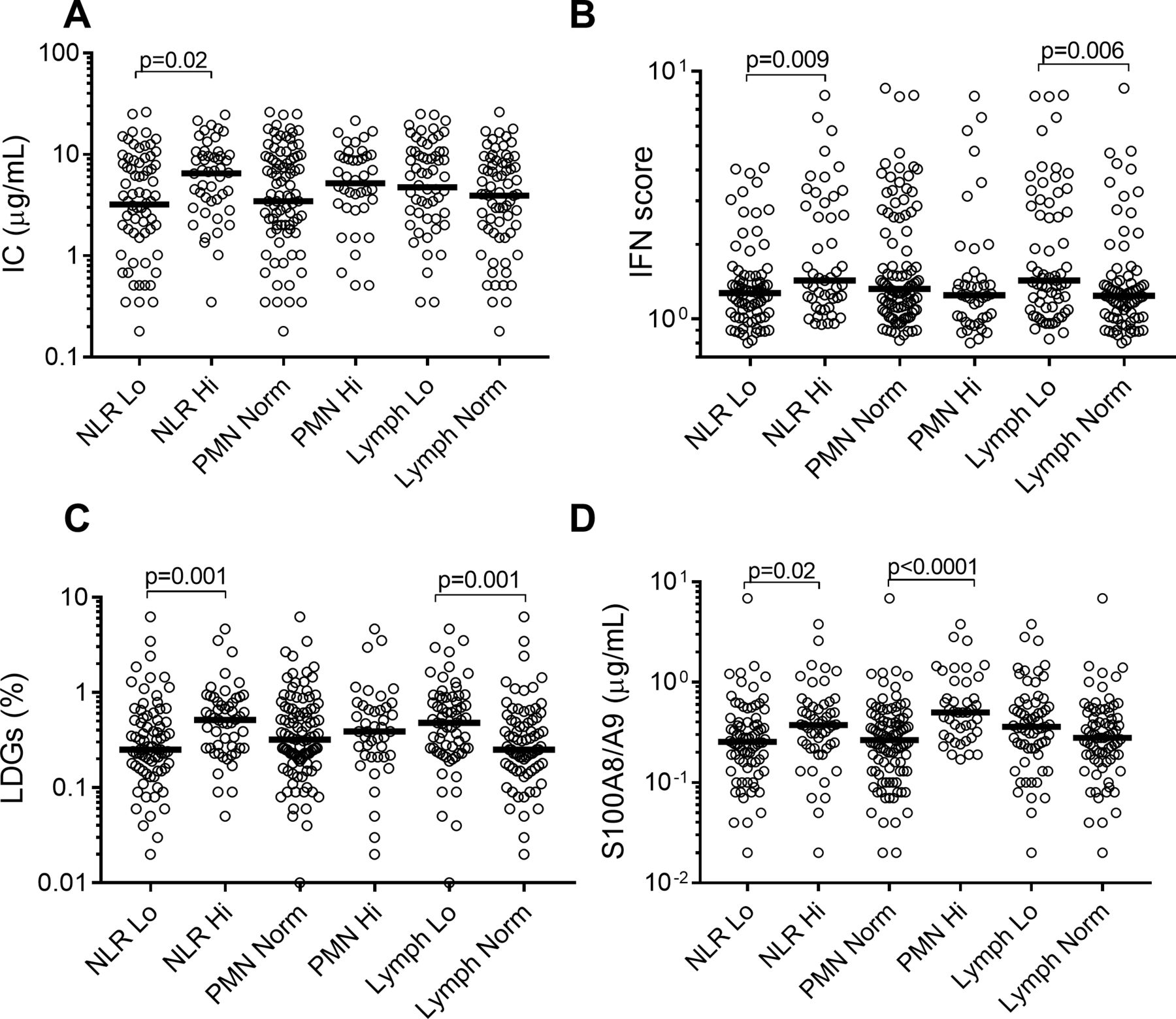
NLR reflects features of both lymphopaenia and neutrophilia. Patients with SLE were stratified based on the level of NLR as high (Hi) versus low (Lo), neutrophils (PMN) as Hi versus normal (norm), and lymphocytes (lymph) as Lo versus Norm. The different groups were compared in their levels of (A) ICs, (B) type I IFN activity, (C) LDGs and (D) calprotectin (S100A8/A9). Statistical analyses were performed using Mann-Whitney U test. ICs, immune complexes; IFN, interferon; LDGs, low-density granulocytes; NLR, neutrophil to lymphocyte ratio; PMN, polymorphonuclear cells.

{kind=link}
{kind=link}
{kind=link}
NLR correlates with immune activation markers. Levels of NLR were correlated with levels of (A) ICs, (B) type I IFN activity, (C) calprotectin and (D) LDGs in patients with SLE. The dotted lines represent the cut-off (2.73) for high NLR, as well as the regression line with 95% CI. All statistical analyses were performed using Spearman’s correlation. ICs, immune complexes; IFN, interferon; LDGs, low-density granulocytes; NLR, neutrophil to lymphocyte ratio.
Associations between markers of neutrophil activation and high NLR
Discussion
NLR is an easily available biomarker reported to have prognostic value in several rheumatic conditions. Consistent with prior work,10 11 we found that NLR was increased in SLE and associated with active disease, as defined by SLEDAI. The association between NLR and disease activity was primarily driven by lymphopaenia, and not neutrophilia. As such, for assessment of disease activity, lymphocyte count may be sufficient. However, as discussed further below, neutrophil count, and in particular NLR, added further insight into the immunopathological mechanisms not captured by lymphocyte count. We did not find any association between NLR and individual disease manifestations, including nephritis, likely due to the overall low disease activity and severity in the cohort. Of note, prednisone use, as well as immunosuppressive drugs were associated with high NLR. Although treatment, including prednisone, may affect neutrophil and lymphocyte counts, it is also plausible that the high NLR levels in these patients reflect a more severe and/or active disease which is more likely to be treated. It was recently reported, using a gene expression approach, that patients with SLE can be stratified into three distinct groups. In two of those groups, neutrophil proportions were associated with SLEDAI, while there was an inverse correlation in the third group.13 Thus, similar to neutrophil counts, NLR may be important in certain subgroups of patients with SLE. Larger cohort studies are needed to further dissect the ability of NLR to identify subgroups of patients with SLE.
A main finding of the current study relates to the association of NLR with LDGs. Recently, LDG to lymphocyte ratio was reported to be better associated with SLEDAI as compared with NLR, suggesting that LDGs may be the main pathogenic subpopulation among neutrophils, consistent with prior work in the field.4 However, in our cohort, we did not find any association between LLR and SLEDAI. Nevertheless, given that LDGs are not routinely analysed in clinical labs, NLR may be a more clinically relevant measure. Surprisingly, the frequency of LDGs was primarily associated with low lymphocyte count rather than neutrophilia, suggesting that LDG production may share the same mechanism that induces low lymphocyte count in SLE.
Asking whether NLR was associated with immunological features of SLE, we made the novel observation that NLR was associated with IC-mediated inflammation, including type I IFN production. The exact mechanism by which NLR is associated with these markers in SLE has not been determined. Nucleic acid-containing ICs bind to FcγRIIA on neutrophils and induce neutrophil activation, including release of NETs, capable of stimulating autoantibody production and downstream IFN production.3 5 Although IC-mediated neutrophil activation may contribute to the elevated levels of calprotectin as well as type I IFNs,5 it is unlikely to account for elevation of NLR, or the disproportionate expansion of LDGs. Instead, our data suggest an indirect association between IC-mediated inflammation and NLR through type I IFNs. Type I IFNs have potent ability to enhance lymphocyte recruitment to tissues, causing lymphopaenia, and stimulate neutrophil activation in bone marrow as seen in SLE.14 Consistent with this interpretation, we found that type I IFN activity was primarily associated with lymphopaenia and not neutrophilia in our study. The association between neutrophil count and calprotectin is intriguing. As shown by us and others, neutrophils are the main producers of calprotectin, with 40% of the cytosolic protein content consisting of calprotectin.15 As such, it is likely that levels of calprotectin, passively (or actively) released by the circulating neutrophil, may be highly associated with neutrophil count. However, recent data also suggest that extracellular calprotectin may act as a neutrophil survival factor, thus promoting their lifespan and accumulation in circulation.16 Further studies are warranted to understand the mechanistic reason for the observed associations.
There are several limitations with the current investigation. First, and foremost, this study is cross-sectional, and therefore it cannot address causality. Additionally, there was a statistically significant difference in immunosuppressive treatment between patients with high and low NLR, which could influence our results. However, the association between NLR and immunological biomarkers remained significant after controlling for prednisone dose and immunosuppressive treatment. A larger longitudinal study including early treatment-naïve patients is needed to evaluate the long-term association between NLR and clinical and laboratory variables, as well as the relationship between NLR and response to treatment in SLE.
In summary, NLR was associated with several immunopathological features of SLE, including type I IFNs and neutrophil activation markers, reflecting both low lymphocyte count and elevated neutrophil count. We also found that NLR had an added value beyond lymphocyte and neutrophil count in reflecting IC-driven disease, which supports NLR as a potential clinically useful and readily available measure in SLE.
Acknowledgments
We are grateful to all the patients who participated in this study.
References
Footnotes
Contributors BKH, KDW and CL designed the study. BKH, AAB, HT and CL contributed with patients and data. KCC advised on the statistical analyses and interpretations. CL and BKH drafted the manuscript. KDW critically revised the manuscript. All authors read and approved the final version of the manuscript.
Funding The study was supported by the Lupus Research Alliance (#519414, CL).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the Institutional Review Board at the Lund University (LU0601450), and informed consent was obtained from all participants.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.