

Abstract
Objective. Fatigue is a frequent, disabling issue in systemic lupus erythematosus (SLE). It is, however, difficult to quantify. The Ad Hoc Committee on SLE Response Criteria for Fatigue in 2007 recommended using the Krupp Fatigue Severity Scale (FSS). Since then, the Functional Assessment of Chronic Illness Therapy (FACIT)-Fatigue Scale has also been validated in SLE. We performed a review of instruments used to measure fatigue in adult SLE patients from 2007 onward.
Methods. We searched PubMed, Medline, and Embase (January 2008–October 2017), identifying clinical trials and observational studies in adult SLE, where fatigue was a specifically measured outcome. All English and French studies were reviewed to determine fatigue measures and results.
Results. Thirty-seven studies met inclusion criteria. Eight scales were used. The visual analog scale (VAS), FSS, and FACIT-Fatigue Scale were most frequent. FSS was the most often used instrument in both clinical trials and observational studies. Twenty-five of the 37 studies demonstrated a difference in fatigue that was statistically significant and clinically meaningful. Of the 12 studies that did not, 6 used FSS, 3 used VAS, 2 used the Multidimensional Assessment of Fatigue, and 1 used the Brief Fatigue Index. All 6 studies using the FACIT-Fatigue Scale detected clinically meaningful and statistically significant differences.
Conclusion. VAS, FSS, and FACIT-Fatigue Scale were the most frequently used instruments in adult SLE studies from 2008 to 2017. Many studies detected clinically important changes in fatigue. Fatigue remains a key measure in both clinical trials and observational SLE studies.
Systemic lupus erythematosus (SLE) is a chronic multi-system autoimmune disorder with significant morbidity and mortality1. Fatigue in SLE is frequent and often debilitating2,3; however, it is a challenging concept to define and measure4,5,6. Numerous instruments have been used in past SLE studies, creating difficulties in interpreting and comparing studies. Because it is a subjective symptom that is difficult to define, fatigue is challenging to measure, which may be why so many instruments exist (a 2007 systematic review identified 71 fatigue-specific instruments available for use in research across all patient populations)7.
In 2007, the Ad Hoc Committee on SLE Response Criteria for Fatigue conducted a systematic review of fatigue instruments used in SLE studies8. They performed a search of articles from 1970 to 2006 and identified 15 instruments. Among these, they recommended the future use of the Krupp Fatigue Severity Scale (FSS) for evaluating fatigue in these patients. It was selected because it was the most frequently used fatigue scale in SLE, had good psychometric properties in patients with SLE, and was validated in multiple languages. In 2011, the Functional Assessment of Chronic Illness Therapy (FACIT)-Fatigue Scale, was also validated in SLE9,10.
The aim of our current study was to perform a review of the instruments used to measure fatigue in adult patients with SLE since the 2007 Ad Hoc Committee recommendations and to summarize fatigue research in patients with SLE over the past 10 years.
MATERIALS AND METHODS
With the assistance of a librarian, we performed a systematic search of PubMed, Medline, and Embase for all English language publications containing MESH terms “systemic lupus erythematosus/SLE” and “fatigue, asthenia, lassitude” (Supplementary material, available with the online version of this article). Our search was further limited to adults. Both clinical trials and observational studies were included. Case reports, reviews, and animal studies were excluded. Given the previous Ad Hoc Committee review article in 20078, we limited our search to articles published between 2008 and October 2017 inclusively. Duplicates were subsequently removed.
Abstracts of the articles obtained with the preliminary search were screened by a single reviewer (AB). After initial screening, full texts were reviewed for inclusion. Publications with a clearly defined adult SLE population, and studying fatigue as a primary or secondary endpoint, were included in our study. Only publications using validated fatigue instruments were retained; studies were excluded if they measured fatigue only through measures of disease activity or quality of life scores (e.g., Medical Outcomes Study Short Form-36). We extracted information from the included studies regarding their design, objectives, and results. In positive studies, we determined whether the results were clinically significant using the minimal clinically important difference (MCID) specific to the instrument used if one was available in the literature.
RESULTS
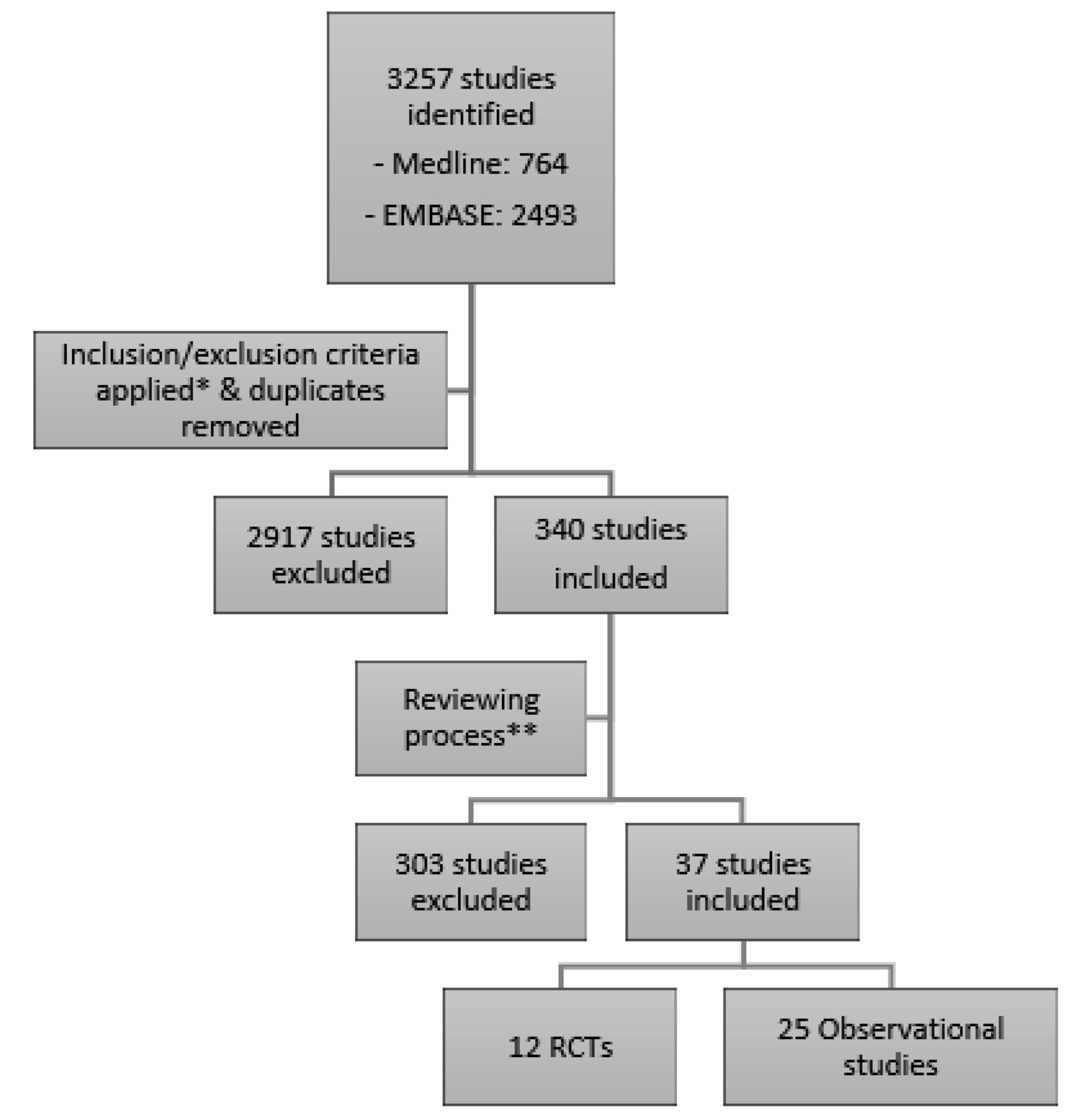
Our search protocol yielded 340 articles after duplicates were removed. Of these, 37 articles met our criteria and were included (Figure 1). Among the 37 studies, 8 fatigue instruments were used (Table 1). The visual analog scale (VAS), Krupp Fatigue Severity Scale (FSS), and FACIT-Fatigue scale were the most frequently used measurements (Table 2, Table 3, and Table 4). The FSS was the most frequently used instrument in both randomized controlled trials (RCT) and observational studies. Twelve of the 37 studies failed to demonstrate a statistically significant difference in fatigue levels related to the exposure of interest. Of these, 6 used the FSS, 3 used the VAS, 2 used the Multidimensional Assessment of Fatigue, and 1 used the Brief Fatigue Inventory (BFI). All 6 studies using the FACIT-Fatigue scale detected clinically meaningful and statistically significant differences. Time until end of followup did not appear to influence study results.

Flowchart of search strategy for selection of included articles. * Case reports, reviews, conference abstracts, and animal studies excluded; search limited to adults and studies in the English language. ** Studies with a clearly defined SLE population, studying fatigue as a primary or secondary endpoint, and using fatigue-specific instruments were included. RCT: randomized controlled trials; SLE: systemic lupus erythematosus.
Fatigue scales used in studies of adults with SLE.
Frequency of fatigue scales overall and subdivided by study type (clinical trial vs observational).
Summary of clinical trials with fatigue as an outcome in SLE.
Summary of observational studies reporting fatigue as an outcome in SLE.
RCT
Among the articles analyzed, 12 consisted of RCT; 5 of these studied the effect of biologic drug therapies on fatigue in patients with SLE. Abatacept was associated with a clinically significant reduction in fatigue compared to placebo at a 12-month followup, using a VAS11. A small RCT of infliximab suggested improvement in fatigue scores but this failed to reach statistical significance in terms of MCID12. Finally, there have been 3 studies each assessing different B-lymphocyte stimulator (BLyS) antagonists. Belimumab, the first BLyS antagonist on the market, was found to have clinically significant improvements in fatigue at 52 weeks of treatment in a phase III study13. Blisibimod was also associated with a significant reduction in fatigue14. A study of tabalumab did not show significant improvement in fatigue scores15. Interestingly, the first 2 studies, showing positive effects on fatigue, used the FACIT-Fatigue scale, whereas the study of tabalumab used the BFI.
Three RCT addressed nonbiologic drug therapies. One RCT studied the effect of N-acetylcysteine (NAC; thought to be by blocking mTOR in T lymphocytes) on disease activity and fatigue. NAC demonstrated a statistically significant reduction in fatigue, using the FAS. Given that the fatigue levels began to rise again during the third month of treatment, the longterm efficacy of NAC is questionable16. An RCT of fish oil did not improve fatigue in SLE17. A placebo-controlled trial involving dehydroepiandrosterone (DHEA) similarly failed to demonstrate improvement in fatigue using the Multidimensional Fatigue Inventory18.
Acupuncture’s benefits on fatigue and pain were studied in a small RCT. There was a trend toward improvement that did not reach statistical significance, possibly due to lack of power19. Two RCT of exercise in SLE demonstrated clinically significant reductions in fatigue. Of note, improvement in fatigue (using the FSS) was noted even in patients with low adherence in one of these studies, raising the question of bias in the intervention group20,21. Low glycemic index and low-calorie diets were also shown to decrease fatigue in SLE patients when measured by the FSS. Statistical significance was achieved with both diets but only the low glycemic index diet met the MCID22.
Observational studies
Twenty-five observational studies were included. As previously described in the literature, patients with SLE were clinically more fatigued compared to age-matched controls23. Regarding predictors, DHEA levels and obesity were not clearly associated with fatigue24,25. One study aimed to identify potential biomarkers for fatigue in patients with neuropsychiatric SLE. It identified a clinically significant association between A proliferation-induced ligand (APRIL) in cerebrospinal fluid and fatigue26. Five observational studies assessing vitamin D levels and fatigue in SLE demonstrated somewhat different results. One study suggested a trend in improved fatigue levels when vitamin D deficiency/insufficiency was corrected with supplementation, but this did not reach statistical significance27. Of the 4 remaining vitamin D studies, 2 demonstrated clinically significant (i.e., met MCID) increased fatigue with low vitamin D levels28,29 while the other 2 were unable to demonstrate associations30,31. Two studies aimed to determine the relationship between muscle strength and fatigue in SLE. One study demonstrated decreased strength with increased fatigue32, while the other was unable to establish this relationship33. Three studies demonstrated a clinically significant association between work disability and fatigue in patients with SLE34,35,36. Finally, lower physical activity, sleep disturbances, pain, anxiety, and depression were all found to be associated with fatigue levels in SLE37–45. Regarding interventions, belimumab was shown to clinically significantly decrease fatigue in patients with SLE in an observational study46. A study of a fatigue and activity management education intervention, administered by occupational therapists, was unable to demonstrate decreased fatigue in SLE47.
Among observational studies, most studies with large sample sizes (> 100) demonstrated a clinically significant change in fatigue29,35,36,37,39–43,45. Smaller studies were unable to demonstrate changes, suggesting that they were underpowered26,28,31,34,48.
DISCUSSION
This review is an important update of instruments used to measure fatigue in SLE in the past 10 years. In this systematic review the VAS, FSS, and FACIT-Fatigue scale were the most frequently used instruments to measure fatigue in adult SLE studies from 2008 to 2017. The VAS is a simple analog scale in which patients mark with an “x” their level of fatigue on a 100-mm line. The advantages are its ease of use and quick administration. Unfortunately, although validated in other populations, this instrument has not yet been studied in SLE and does not consider fatigue’s effect on daily living. Additionally, many studies fail to provide the anchors used with the scale, rendering it difficult to compare their results.
Krupp’s FSS was the most frequently used instrument in our study and was the instrument recommended for use by the 2007 Ad Hoc Committee8. It was designed to measure the effect of fatigue on functional outcomes such as exercise, motivation, and daily activities. It has been validated for use in SLE48.
The FACIT-Fatigue scale is a 13-item questionnaire (originally developed in cancer patients) that measures aspects of physical and mental fatigue and their effects on daily living and functioning. The FACIT-Fatigue scale had not yet been validated in SLE when the Ad Hoc Committee made its recommendations in 2007. The first validation study of FACIT-Fatigue scale in SLE was published in 201110. Like FSS, the FACIT-Fatigue scale has been shown to have good psychometric properties and is easy and quick to administer (< 5 min). Interestingly, all studies that used the FACIT-Fatigue scale found clinically significant associations13,14,23,35,36,37.
The US Food and Drug Administration (FDA) strongly encourages the use of patient-reported outcomes (PRO) as secondary endpoints in SLE clinical trials. Both the FDA and European Medicine Agency emphasize fatigue as being one of the most important PRO to consider. Though no specific scale is recommended, they state that the instrument used should be well defined and have been validated in SLE trial populations49. Difficulty in showing effects of an intervention on fatigue in SLE may well be due to study power for many of the studies that we reviewed.
The FACIT-Fatigue scale and FSS have good construct validity9,50. Both scales have an MCID calculated for patients with SLE51, which allows them to demonstrate changes in fatigue that are both statistically and clinically (in terms of MCID) significant. FACIT-Fatigue scale has been reported to have superior internal consistency and greater sensitivity to change than FSS51. FACIT-Fatigue scale may be more sensitive to detect subjectively important changes in fatigue levels and potentially able to detect a change in smaller sample sizes51. Using focus groups, the FACIT-Fatigue scale has been shown to have good content validity, which means that it appears to be relevant and sufficient for properly assessing fatigue in patients with SLE5,9. The content validity for FSS has not yet been studied52. Fatigue remains an important issue in patients with SLE. Our literature review revealed a small number of clinical trial studies with important reductions in fatigue with medications and nonpharmacologic approaches. Many of these studies used either the FSS, which was recommended for use by the 2007 Ad Hoc Committee, or the FACIT-Fatigue scale, which has demonstrated both superior internal consistency and greater sensitivity compared to FSS51. The VAS, though easy to use and often used in longterm observational studies, has not been validated in SLE and does not record fatigue’s functional effect on patients.
As in any review, our results have potential limitations, and these are partially driven by limitations in the literature. We found that observational studies with larger sample sizes more consistently demonstrated a statistically significant change in fatigue24,29,35,36,37,39–43,45. This suggests that some of the smaller studies included were underpowered26,28,31,34,48. Regarding RCT results, most had a followup time of < 52 weeks, and hence limited our ability to comment on longterm effects.
The VAS, FSS, and FACIT-Fatigue scale were the most frequently used instruments in adult SLE studies from 2008 to 2017. Many studies detected clinically important changes in fatigue. Fatigue remains a key measure in both clinical trials and observational SLE studies. Just as RCT now generally require fatigue scores, fatigue (for example, measured with the FSS or FACIT-Fatigue scale) should be a part of the core data collection for observational SLE studies.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
- Accepted for publication January 17, 2019.








{kind=link}