

Abstract
Objective. To analyze the predictive value of megakaryocyte counts in bone marrow (BM-MK) for determining the therapeutic response of severe thrombocytopenia (TP) in patients with systemic lupus erythematosus (SLE).
Methods. Thirty-five patients with SLE with severe TP (platelet count ≤ 50 × 109/l) from the Peking Union Medical College Hospital admitted between 2007 and 2014 with appreciable bone marrow aspiration results were analyzed retrospectively. The associations between therapeutic response and clinical manifestations, laboratory findings including BM-MK counts, were evaluated.
Results. Seventeen (49%) and 8 (23%) patients achieved a complete response (CR) and a partial response (PR), respectively, and 10 had no response (NR). The BM-MK counts in each group were 102 ± 25 (0–322), 136 ± 48 (2–419), and 28 ± 12 (0–105) per slide, respectively. Significant differences were observed in the counts of BM-MK between patients who achieved a clinical response (CR + PR) and those who did not (NR; p = 0.007). Patients in the NR group exhibited fewer BM-MK compared with those in the CR and PR groups (p = 0.017 and p = 0.006, respectively). A receiver-operation characteristic analysis identified that a cutoff value of BM-MK counts at 20 performed pretty well in discriminating patients with differential responses to immunotherapy, with sensitivity and specificity and area under the curve of 88%, 70%, and 0.798, respectively.
Conclusion. BM-MK count may serve as a good predicting factor for immunotherapeutic response in patients with SLE with severe TP. Patients with BM-MK counts < 20 per slide tend to exhibit poor clinical response.
Systemic lupus erythematosus (SLE) is a classic, diffuse, connective tissue disease that is characterized by multisystem involvement and a diverse autoantibody spectrum1. Hematological involvement is very common. About 10%–40% of patients with SLE develop thrombocytopenia (TP) in their disease course2,3,4,5,6. TP is a reliable marker suggesting active disease5,7. TP may also act as an independent prognostic predictor for end organ damage and higher mortality2,8,9. Refractory TP in SLE is a big challenge that rheumatologists often encounter. Latent risks of fatal bleeding in patients with severe TP justify active immunotherapy. However, the effectiveness of immunotherapy is difficult to predict because of the complicated underlying mechanisms. The presumed mechanisms include platelet destruction and deletion by autoantibodies in the peripheral circulation, inhibition of the development and maturation of megakaryocytes (MK) in bone marrow, consumption of platelets because of thrombotic microangiopathy/thrombotic thrombocytopenic purpura (TMA/TTP), secondary antiphospholipid syndrome (APS), and other miscellaneous causes such as viral infection (e.g., cytomegalovirus, microvirus, Epstein-Barr virus), concomitant hypersplenia, hemophagocytic syndrome (HPS), myelodysplastic syndrome (MDS), aplastic anemia (AA), or myelofibrosis (MF), as well as drug toxicity10,11,12,13. It is essential to discriminate the relevant causes during clinical practice, which necessitates a bone marrow examination to exclude certain hematological disorders. Routine therapeutic interventions for immunological TP include glucocorticoids, immunosuppressive agents [e.g., cyclosporine, tacrolimus (TAC), cyclophosphamide, and mycophenolate mofetil], intravenous immunoglobulin (IVIG), androgens, plasma exchange, rituximab (RTX), and splenectomy14,15. Most physicians and patients prefer pharmacological treatments prior to a splenectomy. However, many patients with SLE with severe TP respond poorly to immunotherapeutic drugs despite careful exclusion of hematological disorders (such as MDS, AA, and MF), TMA/TTP, and hypersplenia. Repeated aggressive treatments may increase the risk of multiple infections and cause considerable economic loss. Therefore, the identification of markers that predict individual responses to immunotherapy is critical. Our retrospective study evaluated whether MK counts in bone marrow (BM-MK) could serve as possible predictive factors for response to immunotherapy.
MATERIALS AND METHODS
Patients with severe TP (platelet count ≤ 50 × 109/l)8 who were admitted to the Peking Union Medical College Hospital between September 2007 and September 2014 and were diagnosed with SLE according to the 1997 American College of Rheumatology SLE classification criteria16 were screened in our study. Patients with concomitant hematological disorders, such as MDS, HPS, or AA, or patients with TMA/TTP, APS, or hypersplenia were excluded. Altogether, 35 patients with SLE with appreciable bone marrow smear results (satisfactory bone marrow sampling, no dilution, no aggregation, and detailed records of the numbers and categories of BM-MK) at the time of TP occurrence were included. Glucocorticoid had been prescribed no more than 2 weeks before bone marrow biopsy was done. Other treatments such as IVIG, disease-modifying antirheumatic drugs, or RTX were not used until bone marrow biopsy results were received. Their clinical data were collected and analyzed. Since our study was based on a review of medical records obtained for clinical purposes, the requirement for written informed consent was waived. This retrospective study was approved by the Peking Union Medical College Hospital Ethics Committee review board. Patients’ information was anonymized and deidentified prior to analysis.
Determination of MK numbers in bone marrow
For all 35 patients, bone marrow were sampled from posterior superior iliac spine, and at least 6 slides of sampled bone marrow smear were prepared with 2 satisfactory slides for Wright-Giemsa staining. Several subtypes of MK can be identified in bone marrow based on morphology, including naked nucleus MK, granulometric MK (GMK), juvenile MK, and platelet-producing MK.
Definition of clinical response
A complete response (CR) was defined as a sustained platelet count equal to or greater than 100 × 109/l for at least 4 weeks during 2 months of therapy. A partial response (PR) was defined as an initial platelet count of 20–50 × 109/l and a sustained platelet count between 50–100 × 109/l for at least 4 weeks during 2 months of therapy. Patients with an initial platelet count < 20 × 109/l and a sustained platelet count of 20–50 × 109/l for at least 4 weeks during 2 months of therapy were also defined as achieving a PR. No response (NR) was defined as the failure to meet the criteria for CR or PR17,18. Relapse was defined as a decrease in platelet count to < 100 × 109/l during followup in patients who had obtained a CR or to < 20 × 109/l for patients who had obtained a PR.
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics software 19 (IBM Corp.). Continuous variables that were normally distributed were compared using ANOVA or the Student t test. Non-normally distributed data were compared using nonparametric tests including the Mann-Whitney U test or the Kolmogorov-Smirnov test. The chi-square test was used to compare differences between categorical variables. The cutoff value was established using the receiver-operation characteristic (ROC) method with the best sensitivity and specificity. The results are presented as means ± standard error of mean (SEM). A p value < 0.05 was considered significant.
RESULTS
General clinical data
The mean age of the 35 patients with SLE with severe TP was 34.3 ± SD 13.6 years (range 11–77). The female to male ratio was 30:5. Twenty-four patients (68.6%) experienced disease onset with TP, and the other patients had a median disease duration of 11 months (range 1–87) prior to TP. Mucocutaneous bleeding occurred in 28 patients (80.0%), and serious visceral hemorrhage occurred in 4 patients (11.4%). The minimum platelet count during the treatment course ranged from 0 to 46 × 109/l (median 4 × 109/l). The median platelet count was 13 × 109/l at the time of bone marrow sampling. Fifteen patients (42.9%) had concurrent leukopenia, and 17 patients (48.6%) had anemia. Thirteen patients (37%) exhibited cytopenia of all 3 cell lineages. Twelve patients (34.3%) had positive anti-dsDNA antibodies, and 14 patients (40.0%) had positive anti-SSA antibodies. The mean SLE Disease Activity Index (SLEDAI) at the time of bone marrow sampling was 6 (range 1–28).
Therapeutic intervention and clinical sequelae
Seventeen (48.6%) and 8 (22.9%) patients achieved CR and PR, respectively, and 10 patients (28.6%) were in the NR group. No significant differences were seen in age, disease duration, clinical manifestations, autoantibody spectrums, or SLEDAI among the 3 groups, except for a relatively higher platelet count before treatment in the CR group (Table 1). Fifteen patients (3 in NR group, 5 in PR group, and 7 in CR group) were examined for platelet-associated immunoglobulin G (PAIgG) titers. Although the NR group seemed to have higher titers of PAIgG, the difference was not convincing because of the small sample size.
Clinical features of 35 patients with SLE and severe TP. Values are % (n) or mean ± SEM unless otherwise specified.
All patients received high doses of corticosteroid (equivalent to prednisone ≥ 0.8–1 mg/kg) in combination with immunosuppressive agents. Fifteen patients (43%) received combined immunosuppressive therapy. Twenty patients (57%) received pulse methylprednisolone (MP) of 0.5–1 g/d for 3 consecutive days. Five of these patients were in the NR group, 7 of these patients were in the PR group, and 8 in the CR group. No differences were observed among the 3 groups regarding the proportion of patients who received pulse MP treatment. Doses of daily steroids were comparable among the 3 groups (CR vs PR vs NR: 80.9 ± 7.1 vs 87.5 ± 8.1 vs 104 ± 14.2 mg/d, p = 0.231; Table 2). Nineteen patients (54%) received IVIG infusion (7, 6, and 6 patients in the NP, PR, and CR groups, respectively). Sixteen patients received a vincristine infusion at least once. Five patients received subcutaneous recombinant thrombopoietin (TPO) injections. RTX was administered in 9 patients (2 in the CR group, 4 in the PR group, and 3 in the NR group). More than half of the patients (18 patients, 51%) in this cohort received a platelet pheresis transfusion. A higher percentage of patients in the NR group received cyclosporine/TAC, as well as platelet pheresis transfusion.
Therapeutic interventions of severe thrombocytopenia among the 3 groups (CR, PR, and NR) in patients with SLE. Values are n (%) or mean ± SEM unless otherwise specified.
Three patients (all in the NR group) died during followup (1–98 mos, median 7 mos). The causes of death were serious infections and SLE relapse. Five patients in the CR group and 1 patient in the PR group had a relapse during followup.
BM-MK and therapeutic responses
Bone marrow smears revealed distinctively active proliferation in 2 patients (5.7%), active proliferation in 28 patients (80%), moderate proliferation in 4 patients (11.4%), and reduced proliferation in 1 patient (2.9%). The BM-MK counts ranged from 0 to 419/slide (median 56/slide). The BM-MK primarily consisted of the GMK subgroup (proportion 76 ± 22.7%, range 0–369/slide, median 42/slide), and this feature was identical among the CR, PR, and NR groups. The BM-MK counts were significantly higher in the CR group (102 ± 25/slide, 0–322/slide) and the PR group (136 ± 48/slide, 2–419/slide) compared with the NR group (28 ± 12/slide, 0–105/slide; p = 0.017 and p = 0.006, respectively; Figure 1). The GMK counts in bone marrow (BM-GMK) of the 3 groups were 84 ± 23, 137 ± 44, and 19 ± 9.5/slide, respectively. BM-GMK counts in patients with clinical responses (CR + PR) were higher than those with no response (p = 0.003; Figure 1).
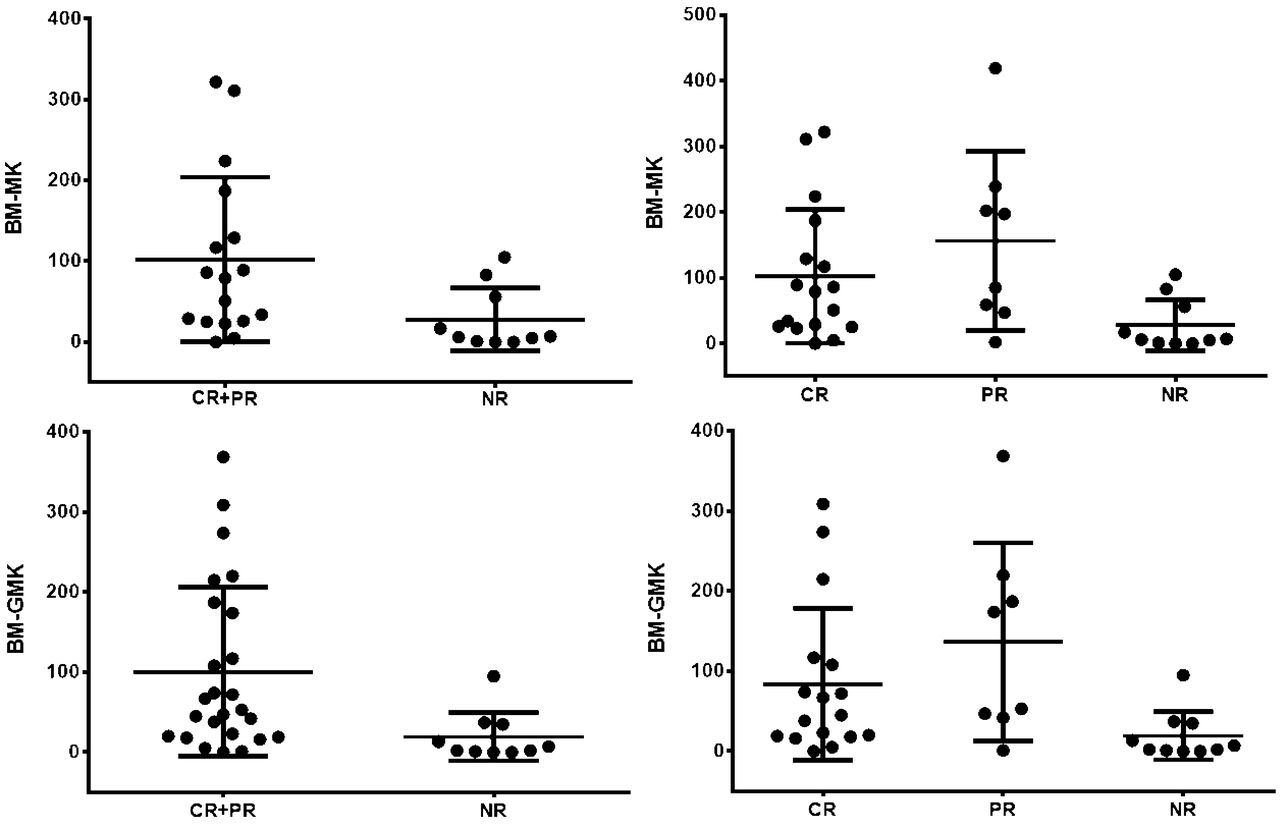
Differential megakaryocyte counts and granulometric megakaryocytes counts in the bone marrow of groups with different clinical responses. BM-MK: megakaryocytes in bone marrow; BM-GMK: granulometric megakaryocytes in bone marrow; CR: complete response; PR: partial response; NR: no response.
To determine whether the number of BM-MK or BM-GMK could contribute to the prediction of patients’ response to treatment, the ROC method was used and the cutoff values of 20/slide for BM-MK and 15/slide for BM-GMK were established, with a sensitivity of 88% and a specificity of 70%. The area under the curve were 0.798 and 0.822, respectively (Supplementary Figure 1, available from the authors on request). The positive predictive value and the negative predictive value were 88% and 70%, respectively. The positive likelihood ratio (LR) was 2.93, and the negative LR was 0.17. When the patients were stratified according to the cutoff value of BM-MK (BM-MK > 20/slide and BM-MK ≤ 20/slide), the effective ratios (CR + PR) were 88% and 30%, respectively (Figure 2). The difference was statistically significant (p = 0.002). We also performed a logistic, stepwise regression analysis, and demonstrated that patients with BM-MK counts > 20/slide were more likely to exhibit a better clinical response (OR 17.11, 95% CI 2.8–104.8, p = 0.002). Average daily dose of steroid immune-suppressants including cyclophosphamide, TAC/cyclosporine, RTX and IVIG, and TPO was not indicative of the clinical responses. Also, in multiple variables logistic stepwise analysis, BM-MK was the only baseline variable that was associated with clinical responses (OR 1.02, p = 0.49); other indices such as SLEDAI, disease course of TP, platelet counts prior to immunotherapy, anti-dsDNA, and hypocomplementemia had no predictive value. One patient repeated bone marrow biopsy 1 month after immunotherapy, and her BM-MK counts before and after treatment were 17 and 9/slide, respectively. This patient was in the NR group with her platelet count continuing to be < 20 × 109/l (Supplementary Figure 2, available from the authors on request).

Clinical responses of patients when stratified with megakaryocytes counts in bone marrow (BM-MK counts ≤ 20 vs > 20). CR: complete response; PR: partial response; NR: no response; BM-MK: megakaryocytes in bone marrow.
DISCUSSION
TP is a common manifestation of patients with SLE, and often predicts poor prognosis7,19. Patients generally receive repeated high-dose steroids and aggressive immune-suppressants to avoid life-threatening hemorrhage. However, a proportion of patients with TP is refractory and may not respond to aggressive immunotherapy, which instead makes the patients vulnerable to severe infections and drug toxicity. Therefore, it is clinically important to identify predicting factors for therapeutic response and avoid unnecessary and inefficacious treatment regimens. Platelets are produced by MK, and TPO is a key growth factor released by MK. An effective TPO concentration is crucial for megakaryopoiesis20,21. TPO binds to its receptor, c-Mpl, and stimulates a downstream signaling cascade, which in turn promotes the development and clonal proliferation and maturation of MK, leading to the final release of platelets22,23,24. Numerous autoantibodies were identified in the peripheral circulation of patients with SLE that can lead to platelet destruction and MK hypoplasia25,26,27. Autoantibodies that are involved in the pathological mechanisms related to TP include PAIgG, anti-CD40 ligand (anti-CD40L), anti-GPIIB/IIIA, anti-TPO, and anti-c-Mpl antibodies28,29,30,31. PAIgG and anti-CD40L contribute to the peripheral destruction of platelets without affecting the production of platelets in bone marrow. Usually these patients had increased or unaltered BM-MK and exhibited a good response to steroid therapy30. However, anti-TPO and anti-c-Mpl antibodies may be involved in amegakaryocytic TP (AMT)25,30,31,32, which correlates to the inhibition of MK clone formation and maturation and decreased MK in bone marrow31,33. It has been reported that patients with anti-c-Mpl antibodies exhibited AMT and significantly poorer response to steroids and IVIG25. The above findings suggest that changes in BM-MK represent a different mechanism of TP and that BM-MK may act as a predictive marker of therapeutic response. Increased MK counts may indicate a better clinical response to immunotherapy, whereas reduced number of MK suggests a poor response.
Our cohort excluded patients with complex factors, such as TTP, APS, HPS, MDS, and AA. Only patients with appreciable bone marrow smear results and detailed MK information were included because we planned to focus on BM-MK. All patients received high-dose steroids and single or combined immunosuppressive agents, including RTX treatment in 9 patients. The results showed that patients with positive clinical responses had higher BM-MK counts than those who did not respond, and this difference was statistically significant. Examinations of anti-TPO and anti-c-Mpl antibodies were not routinely performed. Therefore, we did not have the data to evaluate the correlations between reduced BM-MK counts and these autoantibodies. Therapeutic intensity was comparable among the 3 groups with different clinical responses, or even more aggressive therapy was given to patients in the NR group. Consistent with our hypothesis, reduced MK counts in bone marrow were associated with poor response to treatment. Our study also found that the ROC analysis with a cutoff value of 20 BM-MK performed well in discriminating between responders and nonresponders, with sensitivity and specificity of 88% and 70%, respectively. A logistic stepwise regression analysis demonstrated that only stratification based on the number of BM-MK, but not the type of treatment intervention, was indicative of clinical response. Because TPO-receptor agonist drugs such as romiplostim and eltrombopag are promising effective treatments in refractory TP and AMT in patients with SLE34,35, those with severe TP who have significantly decreased BM-MK should receive TPO-receptor agonist treatment more readily.
Our study had limitations. It was retrospective, and only patients with appreciable bone marrow results were included; thus selection bias is possible. The followup time was also short and varied from patient to patient. We did not stratify patients according to the treatment regimens they received because of the limited sample sizes. TP attributable to AMT in patients with SLE that is resistant to routine therapeutic measures may respond to RTX18,36,37, but the benefits of RTX treatment were not overwhelmingly significant in our study.
Our study suggests that the number of BM-MK may be a good predictor of patients with SLE’s response to immunotherapy. Multi-loci sampling of bone marrow may be required for better evaluations because MK counts in bone marrow may not be uniformly distributed.
- Accepted for publication February 18, 2016.








{kind=link}
{kind=link}