Article Text

Abstract
Background Although case series suggest a higher burden of cardiovascular risk factors in patients with systemic lupus erythematosus (SLE) compared with the general population, the association between SLE and heart failure (HF) remains undefined. We sought to investigate the incidence and risk of HF in patients with SLE.
Methods In April 2016, we performed a retrospective cohort analysis using the Explorys platform, which provides aggregated electronic medical record data from 26 major integrated healthcare systems across the USA from 1999 to present. Demographic and regression analyses were performed to assess the impact of SLE on HF incidence.
Results Among 45 284 540 individuals in the database, we identified 95 400 (0.21%) with SLE and 98 900 (0.22%) with a new diagnosis of HF between May 2015 and April 2016. HF incidence was markedly higher in the SLE group compared with controls (0.97% vs 0.22%, relative risk (RR): 4.6 (95% CI 4.3 to 4.9)), as were other cardiovascular risk factors. In regression analysis, SLE was an independent predictor of HF (adjusted OR: 3.17 (2.63 to 3.83), p<0.0001). RR of HF was highest in young males with SLE (65.2 (35.3 to 120.5) for age 20–24), with an overall trend of increasing absolute risk but decreasing RR with advancing age in both sexes. Renal involvement in SLE correlated with earlier and higher incidence of HF.
Conclusions The findings of this study suggest that patients with SLE have significantly higher risk of developing HF and a worse cardiovascular risk profile compared with the general population. These results need to be confirmed by prospective studies.
Statistics from Altmetric.com
Introduction
Limited data suggest an increased risk of heart failure (HF) in patients with systemic lupus erythematosus (SLE) compared with the general population.1 While many studies have linked rheumatological conditions to coronary artery disease (CAD)2 ,3 and identified it as a major cause of morbidity and mortality in patients with SLE,4 long-term data show that only about 20% of HF in patients with SLE is attributable to CAD, suggesting that other factors play a role.5 SLE has also been associated with a higher burden of traditional cardiovascular risk factors including hypertension, diabetes mellitus, smoking, dyslipidaemia and obesity,6–8 though it has been suggested that the impact of these traditional risk factors in patients with SLE may be different compared with the general population.9 While patients with SLE have experienced improved overall survival over the past 30 years due to advances in SLE treatment, their cardiovascular mortality remains largely unchanged,10 highlighting an opportunity for intervention. In this study, we sought to investigate the incidence and risk of HF in patients with SLE and determine their cardiovascular risk profile.
Methods
Study design and population
In April 2016, we queried a large, multi-institutional commercial electronic healthcare database (Explorys, Cleveland, Ohio, USA)11 to perform a retrospective cohort analysis. The Explorys platform (EPM: Explore) provides aggregated electronic medical records from outpatients and inpatients from 26 major integrated healthcare systems spanning all 50 states in the USA, capturing data from over 48 million patients from 1999 to present. Clinical information from multiple sources, including electronic medical records, practice management systems, as well as billing, lab, scheduling and claims systems, is matched via a proprietary engine to create longitudinal records for each unique patient. The data are standardised and curated in the database according to common clinical standards such as the International Classification of Diseases, Systemized Nomenclature of Medicine—Clinical Terms (SNOMED-CT), Logical Observation Identifiers Names and Codes and RxNorm. The Explorys search engine provides an interactive platform in which its millions of unique patient and clinical data elements are open to search, browse and analysis functions. Population counts are reported to the nearest 10, or represented as <10 if between 0 and 10, to prevent patient identification.
All 45 284 540 non-deceased patients in the database at the time of our query were included in this study, among which we identified 95 400 patients with SLE. There were 98 900 patients and 828 830 patients with a new diagnosis of HF during the preceding 1-year (May 2015–April 2016) and 10-year (May 2006–April 2016) periods, respectively. SNOMED-CT terms ‘heart failure’ and ‘systemic lupus erythematosus’ were used to broadly identify those with HF and SLE, respectively. Patients with other cardiovascular risk factors, including advanced age, male sex, hypertension, diabetes mellitus, tobacco use, dyslipidaemia, obesity and family history of CAD, were identified using the search terms ‘demographic: senior’, ‘gender: male’, ‘diagnosis: hypertensive disorder’, ‘diagnosis: diabetes mellitus’, ‘finding: smoker’, ‘diagnosis: disorder of lipoprotein storage and metabolism’, ‘diagnosis: obesity’ and ‘family history: cardiovascular disease’, respectively. A complete list of search terms is given in online supplementary table S1. This study did not require a separate review by the institutional review board as it only included aggregated, de-identified population data.
Supplementary tables
Statistical analysis
Population counts were recorded to the nearest 10, or as 5 for counts reported as <10. Data were imported and analysed using the R statistical software package (V.3.2.3 for Windows, R Foundation for Statistical Computing, Vienna, Austria). We report conservative estimates of the annual incidence of HF by age, sex and disease status, as well as relative risk (RR) of HF by age category. For the baseline cohort, we estimated the population at risk in May 2015 by the number of non-deceased individuals in the Explorys database in April 2016, while acknowledging the limitations arising from the increase in the number of distinct individuals in the database over time versus deaths occurring during this period. For incident cases of HF, we identified the number of newly reported HF diagnoses during the preceding 1-year period (May 2015–April 2016), while for estimation of RR of HF by age category, we used the yearly average of the number of newly reported HF diagnoses during the preceding 10 years (May 2006–April 2016) for increased sensitivity. We also report the prevalence of cardiovascular risk factors and their respective RRs by disease category. All RRs and 95% CIs were computed according to Altman.12
To assess the impact of SLE among other cardiovascular risk factors on the development of HF, multiple logistic regression analyses were performed. The main regression model evaluates SLE against the most common risk factors for HF, including advanced age, CAD, previous myocardial infarction, hypertension, valvular heart disease, as well as common confounders of HF in this population, including anaemia and chronic kidney disease. Manual variable selection was performed to test for and include the most significant interactions between SLE and other risk factors for HF. In addition, SLE was evaluated against traditional atherogenic risk factors, as well as a more finely graded age variable. Finally, to evaluate whether the risk of HF varies among subgroups within the SLE population, the copresence of SLE and nephritis was used as a proxy for more severe SLE, and compared against patients with SLE without nephritis. Given the unavailability of individual-level data in the Explorys database, we determined separate event rates for each combination of binary variables (including dummy variables for age-graded analysis) to perform multiple logistic regression. Independence between predictors was assessed using the variation inflation factor (VIF), with cut-off for significant collinearity set at VIF >1.5. Goodness of fit for regression models was assessed via Pearson's χ2 statistic. All statistical significances were set at p<0.05.
We performed several sensitivity analyses to evaluate the robustness of our inferences. For identifying HF cases, we considered all coded HF diagnoses reported in the 1-year period preceding the time of our query, all coded cases of new HF diagnoses made in the preceding 1-year period and coded cases of new HF diagnoses averaged over the preceding 10-year period. In addition, we assessed whether application of the Framingham HF diagnostic criteria13 would improve the specificity of the identified HF diagnoses, by including clinical characteristics as additional qualifiers for HF diagnosis (see online supplementary table S2). This was performed by including 1, 2 or 3 Framingham criteria as additional requirements to the SNOMED-CT search term ‘heart failure’ to qualify as a HF case in the Explorys search platform. These candidate HF diagnoses were then compared against figures reported in previously published epidemiological studies on HF incidence to assess their sensitivity and specificity in identifying HF cases. Based on these comparisons, we elected to use new diagnosis of HF in the preceding 1-year period for estimation of annual incidence, new diagnosis of HF averaged over the preceding 10-year period for estimation of age-specific RR of HF and all coded HF diagnoses in the preceding 1-year period for multiple regression analysis.
Results
Among 45 284 540 unique, non-deceased individuals in the database at the time of our query, we identified 95 400 (0.21%) patients with SLE (SLE group) and 45 189 140 patients without SLE (control group). There were 98 900 patients and 828 830 patients with a new diagnosis of HF during the preceding 1-year (May 2015–April 2016) and 10-year (May 2006–April 2016) periods, respectively.
Incidence and risk of HF
Annual incidence of HF was markedly higher in the SLE group compared with the control group (0.97% vs 0.22%, RR: 4.6 (95% CI 4.3 to 4.9)) (table 1). Overall HF risk with SLE was slightly higher in males compared with females (RR: 6.3 (95% CI 6.0 to 6.7) vs 5.0 (95% CI 4.8 to 5.1)). In males with SLE, while the absolute risk of HF increased with age, RR of HF was markedly higher in younger age groups, with RR of 65.2 (95% CI 35.3 to 120.5) for age 20–24, 53.8 (95% CI 35.0 to 82.7) for age 25–29, 36.7 (95% CI 25.9 to 52.1) for age 30–34 and 17.8 (95% CI 12.5 to 25.3) for age 35–39. A similar trend of increasing absolute risk but decreasing RR with advancing age was also seen in females, with RR of 49.5 (95% CI 37.3 to 65.6) for age 20–24, 33.2 (95% CI 27.4 to 40.1) for age 25–29, 22.4 (95% CI 19.1 to 26.2) for age 30–34 and 15.8 (95% CI 13.9 to 18.0) for age 35–39. These trends are illustrated in figure 1.
Incidence and risk of HF by age, sex and disease status
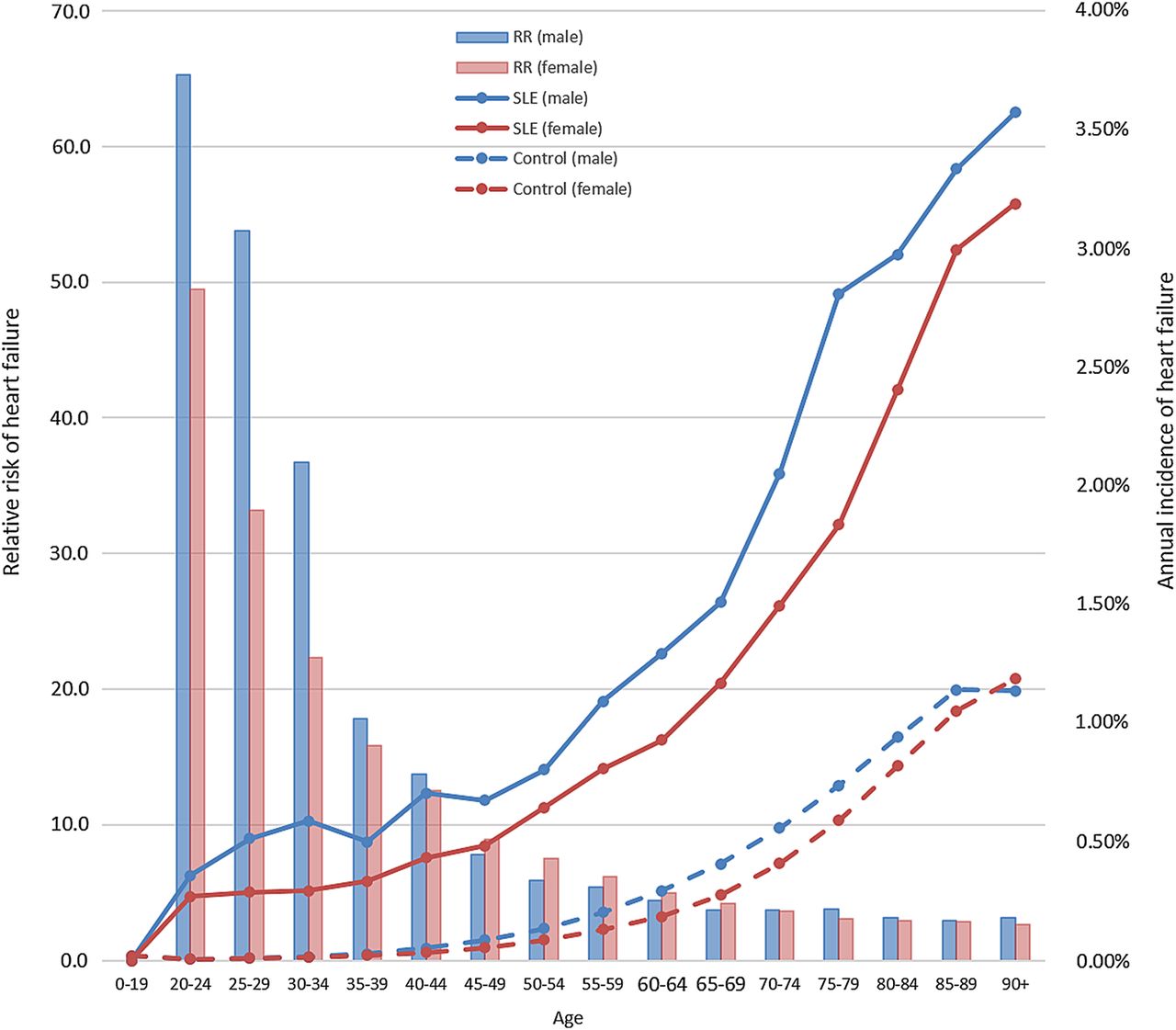
Annual incidence and RR of heart failure over age, by sex and disease status. RR, relative risk; SLE, systemic lupus erythematosus.
Prevalence of cardiovascular risk factors
Prevalence of cardiovascular risk factors is shown in table 2. Most cardiovascular risk factors were significantly more prevalent in the SLE group, including advanced age (23.5% vs 19.1%), hypertension (50.8% vs 16.3%), diabetes (18.2% vs 6.3%), smoking (22.9% vs 9.2%), dyslipidaemia (35.4% vs 13.4%), obesity (19.3% vs 5.3%) and family history of CAD (8.5% vs 2.0%). Other common risk factors of HF were also more prevalent in the SLE group, including CAD (12.6% vs 3.9%), valvular heart disease (11.2% vs 2.2%), conduction system disease (21.9% vs 6.0%), pulmonary hypertension (2.2% vs 0.2%) and thyroid disease (28.6% vs 6.2%). Aside from age, sex and race, unadjusted RR for all examined risk factors were at least twice as high for the SLE group compared with the control group.
Prevalence of cardiovascular risk factors by disease status
Predictors of HF
Results of the multiple logistic regression models, with HF as the response variable, are shown in table 3. Controlled against common risk factors for HF, SLE was an independent predictor of HF (adjusted OR: 3.17 (95% CI 2.63 to 3.83)). Hypertension was the strongest predictor of HF (OR: 12.26 (95% CI 12.07 to 12.46), followed by valvular heart disease (OR: 3.20 (95% CI 3.17 to 3.24)) and CAD (OR: 2.84 (95% CI 2.79 to 2.86)). This relationship persisted when compared against more finely graded age groups (see online supplementary table S3). Controlled against other atherogenic risk factors, SLE remained an independent predictor of HF (OR: 2.01 (95% CI 1.94 to 2.08)). There was little collinearity between factors, where all computed values for VIF were <1.5, except between graded age groups. p Values for Pearson's χ2 goodness-of-fit test were >0.05 in all models, indicating good fit. Finally, when the presence of nephritis was used as a proxy to represent more severe SLE activity, there was a marked, graded difference in HF incidence between those with SLE with nephritis versus SLE without nephritis versus without SLE (figure 2).
Multiple logistic regression results

Annual incidence and RR of heart failure over age, by the presence of nephritis. RR, relative risk; SLE, systemic lupus erythematosus.
Discussion
In an unprecedented comparison of almost 100 000 patients with SLE to more than 45 million controls, we show that the incidence of HF is almost five times higher in patients with SLE compared with the general population. We also confirm that cardiovascular risk factors are more prevalent in patients with SLE. While prior studies have focused on specific cardiovascular events such as myocardial infarction and cardiovascular death, data pertaining to HF as an independent outcome are scarce.5 ,14 ,15 To our knowledge, this is the first large-scale study to examine risk factors for HF in patients with SLE.
Here, we show that SLE is an independent risk factor for HF, conferring over twofold increase in adjusted overall risk in multiple regression analysis. Despite the increased prevalence of cardiovascular risk factors in the SLE population, we found that SLE is a stronger predictor of HF than diabetes, smoking or dyslipidaemia. Increased risk of HF was particularly pronounced in younger patients with SLE, with more than 20-fold increase in RR among patients under the age of 35, and reaching up to over 50-fold risk in patients under 25. These represent a much higher risk than previously reported, and particularly so for young males with SLE, for whom risk of HF has not been previously described. This relationship was consistently observed across different definitions of HF within the Explorys database (figure 3). This is in comparison to a study by Ward,14 where young women (age 18–44) with SLE had an OR of 3.80 (95% CI 2.41 to 5.19) for hospitalisation due to HF, among an overall trend of increasing absolute risk of HF but decreasing RR over advancing age. Such disproportionately elevated risk of HF in young patients strongly suggests a pathophysiological relationship between SLE and development of HF.

Comparison of relative risk of heart failure by the definition of heart failure.
The mechanisms underlying the elevated risk of HF, especially in younger patients, remain speculative. While direct myocardial involvement in SLE has been documented,16 lupus myocarditis is rare and does not explain the high HF risk found in this study. However, the observed risks are likely due to a combination of microvascular disease and chronic inflammation. Accelerated vascular disease has long been described in SLE, which is partly mediated by dyslipidaemia, vascular epidermal growth factor and oxidative stress, promoting the development of coronary plaques.17 In addition, direct myocardial effects of inflammatory cytokines may also play a role in the development of non-ischaemic cardiomyopathy in these patients. For example, tumour necrosis factor α and interleukin-6, both elevated in SLE,18 ,19 have been shown to reduce ventricular contractility and lead to HF20 ,21 in animal models, and their association with HF has been confirmed in SLE.22 Our regression model results also suggest significant interplay between SLE and common HF risk factors. Such heterogeneous aetiology is also suggested by prior studies. In an analysis of a multinational SLE cohort of 1242 patients, Urowitz et al5 reported that among 24 cases of HF identified, only 5 (20.8%) were attributable to CAD, while 12 (50.0%) were attributed to active SLE and 7 (29.1%) to other causes, suggesting a multifactorial aetiology to HF in patients with SLE. Further studies are needed to elucidate mechanisms underlying elevated HF risk in SLE.
In our study, the most prevalent risk factors for HF in the SLE population were hypertension, dyslipidaemia, anaemia, thyroid disease and conduction system disease, while the largest discrepancies in prevalence between the SLE and control groups occurred in pulmonary hypertension, chronic kidney disease, amyloidosis, anaemia and valvular heart disease. These results are consistent with previously reported findings in the LUMINA lupus cohort, where there was increased prevalence of pulmonary hypertension (2.2%–9.3%), kidney disease (38.6%–41.9%) and valvular heart disease (6.6%–39.5%).15 In another study of 69 patients with SLE and 56 controls followed by serial echocardiography, Roldan et al23 reported an overall prevalence of valvular heart disease of 61% in patients with SLE versus 9% in controls, where many valvular abnormalities were seen to resolve or appear anew over time. While temporally unrelated to other SLE manifestations, valvular heart disease was related to cardiovascular events, including HF (13% vs 0%, p=0.03),23 consistent with our findings.
While the increased risk of cardiovascular risk factors and adverse outcomes in patients with SLE is known, there have been no sufficiently powered clinical trials to guide cardiovascular risk management in patients with SLE. Furthermore, it is not known whether modification of traditional cardiovascular risk factors in patients with SLE will affect cardiovascular disease outcomes as in the general population. While the American College of Rheumatology recognises SLE as an independent risk factor for accelerated atherosclerosis and recommends tight blood pressure control for all patients with SLE with a target blood pressure <130/80 (level A) and statin therapy for all patients with SLE with low density lipoprotein >100 mg/dL (level C),24 it should be noted that aside from general cardiovascular risk, there are currently no recommendations specific to HF. Future studies that address the increased risk of HF in patients with SLE are needed.
Limitations
There are several limitations to this study and our results are preliminary. First, it is retrospective in design, with its inherent biases and confounding. Second, there are intrinsic limitations to an aggregated electronic medical record database, where diagnoses are based on charted codes and only limited collateral clinical data are available. Within the Explorys platform, individual-level details such as the date of diagnosis, diagnostic modality and timeline of events are lost and numbers are rounded to the nearest 10, causing distortion when dealing with rare events. Whereas we tried to infer causality of events by specifying temporal relationships between diagnoses, it is possible that some risk factors were identified after the diagnosis of HF. There is also systematic under-representation of disease subcategories in an aggregated database, due to incomplete and/or non-specific coding. For HF, current classification system of HF with reduced ejection fraction or HF with preserved ejection fraction were not reflected in the database, nor was classification by systolic or diastolic HF specified for the majority of patients. Due to this limitation, we chose all-inclusive HF, rather than a specific type of HF, as our primary outcome variable.
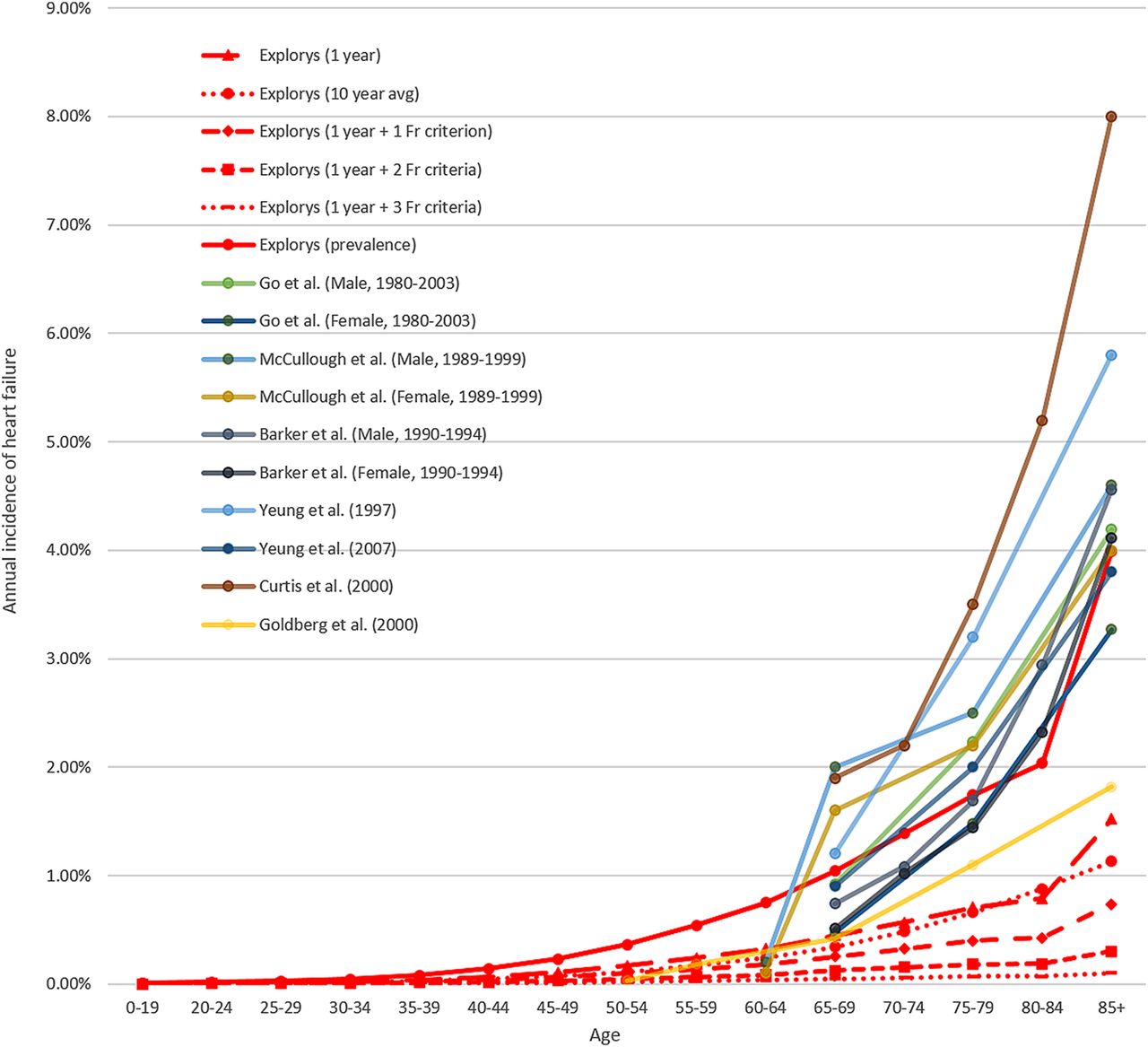
We indirectly verified the validity of HF diagnosis within the Explorys database by comparing HF incidence against previously published data (figure 4),13 ,25–29 though we elected not to incorporate additional Framingham criteria as part of our HF definition due to the large loss in sensitivity. This lack of sensitivity is not unique to the Explorys database; in a recent meta-analysis, McCormick et al30 reported that in identifying HF in administrative databases, overall sensitivity was only around 65%, while specificity exceeded 95%. Even so, the validity of diagnostic codes in the Explorys database has not been specifically evaluated, and as such there exists potential for misclassification error. Finally, in our examination of risk factors for HF, we did not include SLE severity or medical therapy, specifically corticosteroids and other immunomodulators that are known to affect cardiovascular risk,2 ,6 due to the lack of available details regarding timeline, dosing and adherence. Such omission could have had significant impact on the estimation of effect size in our regression models. Therefore, prospective controlled cross-sectional and longitudinal studies are needed to validate these results.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of heart failure incidence by the definition of heart failure.
Conclusions
The findings of this study suggest that patients with SLE have significantly higher risk of developing HF and a worse cardiovascular risk profile compared with the general population. These results need to be confirmed by prospective studies.
Key messages
What is already known on this subject?
Previous studies have shown a higher burden of cardiovascular risk, including accelerated atherosclerosis and increased incidence of major cardiovascular events, in patients with systemic lupus erythematosus (SLE) compared with the general population.
What might this study add?
The association between SLE and heart failure (HF) remains undefined, as very few studies have examined HF as the primary outcome. We therefore sought to investigate the incidence and risk of HF in patients with SLE.
How might this impact on clinical practice?
Our results show remarkably elevated risk of HF in patients with SLE, particularly in those who are young. Once these findings are validated by prospective studies in the future, more aggressive screening for HF may be indicated in this population.
References
Footnotes
Contributors CHK: design of study, data collection, analysis and drafting of manuscript. SGA-K: data analysis and manuscript revision. BJ, ADA and MZ: manuscript revision and guideline review. GHO: supervisor of study and manuscript revision. The authors confirm that the manuscript is an honest, accurate and transparent account of the reported study.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.