Article Text

Statistics from Altmetric.com
Pulmonary arterial hypertension (PAH) is a severe complication of systemic lupus erythematosus (SLE), and SLE-PAH is the most common connective tissue disease (CTD)-associated PAH in Chinese patients.1 The prognosis of SLE-PAH is poor, with 3-year survival rates varying from 45% to 88%.2 3 Due to the complexity and heterogeneity of the underlying disease, it is necessary to further differentiate among SLE-PAH patterns to better understand the disease and optimise its management.
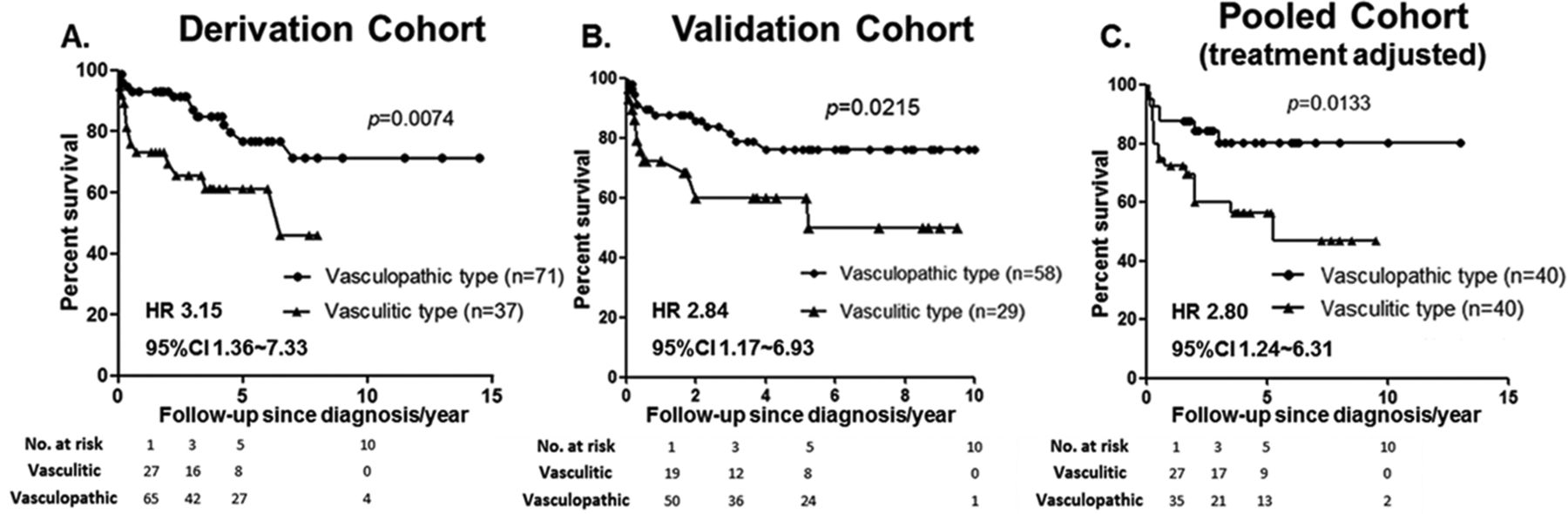
Between 2011 and 2016, a derivation cohort (Shanghai Ren Ji Hospital, n=108) and a validation cohort (Guangdong General Hospital, n=87) of patients with SLE-PAH from two medical centres were included. Patients with SLE-PAH were diagnosed based on right heart catheterisation or echocardiography (peak tricuspid regurgitation velocity >3.4 m/s), and those with left heart disease, pulmonary thrombosis and lung diseases were excluded.4 Based on the baseline clinical manifestations and laboratory findings at the time of the diagnosis of PAH, two distinct clusters were identified and validated by multiple correspondence analysis and k-means clustering. Cluster 1 had systemic manifestations and high SLE disease activity, including pericarditis, rash, arthritis, nephritis and neuropsychiatric lupus, while cluster 2 tended to have low disease activity but purer PAH. According to their characteristics, cluster 1 and cluster 2 were named the vasculitic subtype and the vasculopathic subtype, respectively. Kaplan-Meier survival analysis revealed that patients with the vasculitic subtype had a significantly higher 3-year mortality rate than those with the vasculopathic subtype (34.5%–40.2% vs 13.0%–18.6%, p<0.05; HR 2.84–3.15). The difference in survival still existed after adjusting for treatment variations, including corticosteroids, immunosuppressants and PAH-targeted vasodilators, by propensity score matching (figure 1), which further underscores the importance of two clinical phenotypes. To identify predictors of the high-risk vasculitic subtype, multivariate logistic regression was performed and optimal cut-offs were obtained by receiver operating characteristic curve. The time interval between the diagnoses of SLE and PAH (<2 years, p<0.0001) and the Systemic Lupus Erythematosus Disease Activity Index (SLEDAI >9, p=0.001) score were identified as two independent predictors in both cohorts. A prediction model combining these two factors was further developed and a weighted score ≥2 yielded a sensitivity of 98.5% and a specificity of 74.4% (area under the curve 0.94, p<0.0001) in discriminating the vasculitic subtypes (table 1).

{kind=link}
Survival curves for patients with systemic lupus erythematosus-pulmonary arterial hypertension in two distinct clusters from two independent cohorts (A and B) and the pooled cohort (C). Pooled cohort (C) was derived by propensity score matching according to different treatments.
Parameters of the prediction model in the derivation, validation and pooled cohorts
To the best of our knowledge, this is the first study aiming to distinguish between different clinical phenotypes of SLE-PAH in two independent cohorts. A simple and reliable prediction model was developed, which yielded a high predictive performance for the high-risk vasculitic subtype. Of the two predictors identified in this study, SLEDAI scores are widely used to evaluate SLE disease activity, and the categories of ≤4, 5–9 and >9 are clinically meaningful to represent low, moderate and high overall SLE activity, respectively. Interestingly, early onset of PAH after the diagnosis of SLE was a newly identified predictor of the vasculitic subtype in our study. It has been reported that patients with a simultaneous diagnosis of PAH and CTD are more likely to have active underlying disease and are prone to respond to intensive immunosuppressive therapy.5 It is noteworthy that this dichotomisation and nomenclature was based on clinical rather than pathological characteristics. Nevertheless, the existence of distinct clinical phenotypes of SLE-PAH hypothetically suggests different underlying pathophysiological mechanisms, that is, autoimmune-mediated processes versus non-inflammatory vascular remodelling.6 However, the clustering of patients with SLE-PAH found in this retrospective study needs further confirmation in prospective studies. The next key question that remains unanswered is how to balance the utility of immunosuppressants and PAH-targeted drugs in patients with different phenotypes. The results of our study may help facilitate the individualisation of disease management and guide future clinical trial design in patients with SLE-PAH.
Footnotes
FS and YL contributed equally.
Handling editor Josef S Smolen
Contributors All authors took part in drafting and revising the article, and all authors approved the final version to be published. XZ and SY had full access to all the data in the study and take responsibility for the integrity and accuracy of the data. Study design: XZ and SY. Acquisition of data: FS, YL, WW and LG. Analysis and interpretation of data: FS, YL and WW.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests SY has received research funding from the National Key Research and Development Program of China. FS has received research funding from Ren Ji Hospital South Campus, School of Medicine, Shanghai Jiao Tong University. Other coauthors have nothing to disclose.
Patient consent Not required.
Ethics approval The ethical approval was waived for this study due to its retrospective design.
Provenance and peer review Not commissioned; externally peer reviewed.