

To the Editor:
Recent reports have suggested that in spite of rheumatology-specific research in the area, there remained a need for further research and development of transitional care for adolescents reaching adulthood, as highlighted in an editorial and paper in this journal1,2. In the United States, “Six Core Elements of Health Care Transition” have been defined by the federally funded national resource center on transition (Got Transition)3. McManus, et al recently reported a study that observed improvements in all 6 transition quality indicators when these elements were addressed in the clinical setting4.
Informational continuity is 1 of several continuities recognized as important in transitional care5 and is reflected in several of the core elements referred to above3,4. Although a medical summary3 as described in core element No. 4 was ranked in the top 2 aspects of successful transition by adult physicians6, only 16% of the North American Childhood Arthritis and Rheumatology Research Alliance (CARRA) members reported as having helped with the creation of a medical summary2. Coordinated transitional care, however, has been reported to significantly improve with the provision of such information4,7.
We recently carried out a retrospective departmental case note review8 of all transferred patients during the last 5 years from a department that has an established transitional care program9.
Two hundred forty-two patients were identified. Of them, 152 were transferred to 35 rheumatologists and 90 were discharged to primary care. Of the patients transferred, the mean age (SD) at diagnosis was 10 years (1–16) and the mean age at transfer was 17 years (16–19). Sixty-four percent were women (n = 97) and 26% were nonwhite (n = 39). Sixty-nine percent had juvenile idiopathic arthritis (n = 105) and 59% were receiving a disease-modifying antirheumatic drug (DMARD)/biologic during transfer (n = 89). Thirty-seven percent had a comorbidity (n = 56).
The median (mean, range) duration between the last pediatric and the first adult appointment was 115 days (102, 0–457; Figure 1). Thirteen patients were lost to followup, including 11 with inflammatory disease, 4 with comorbidities, and 3 receiving a DMARD or a biologic.
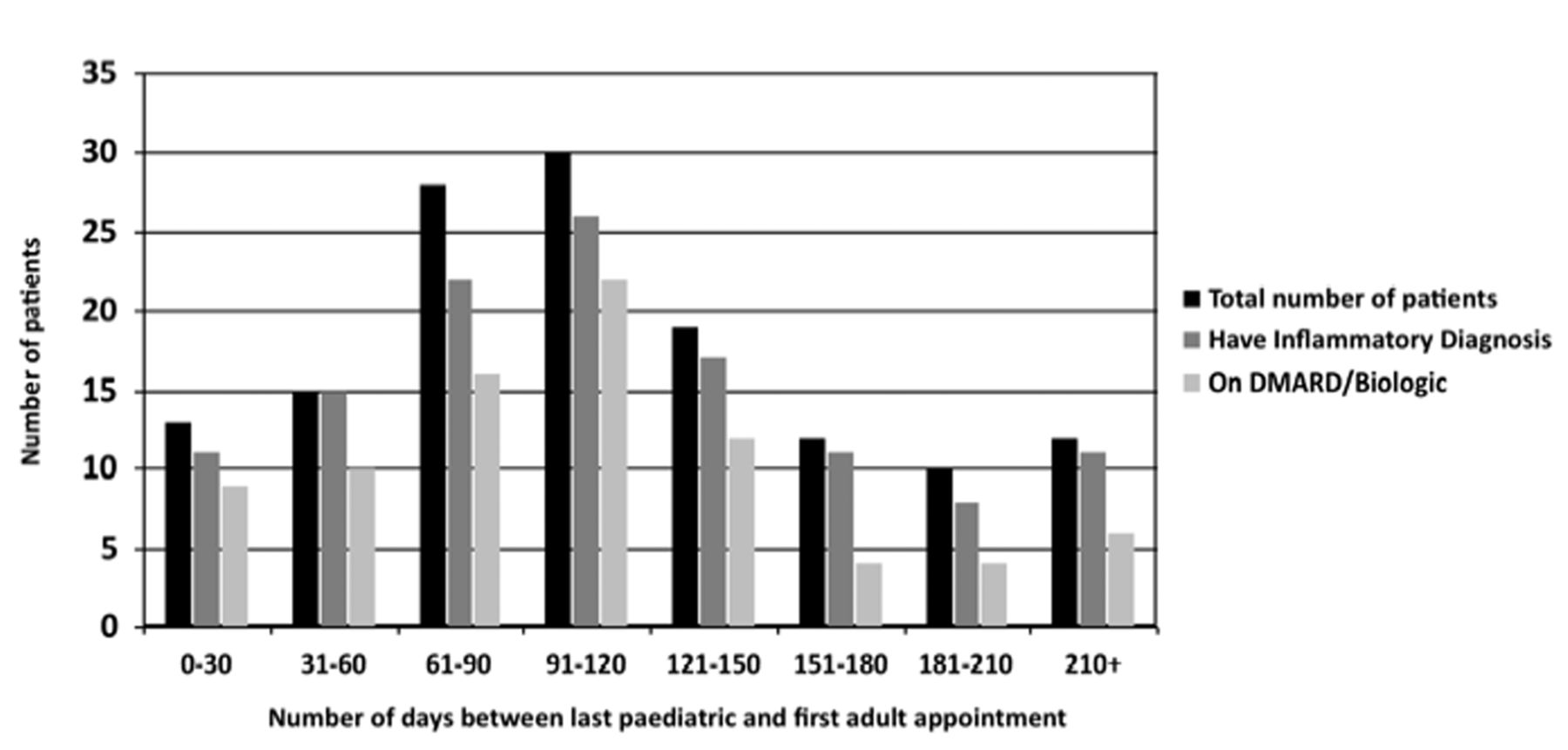
Duration (in days) between last pediatric clinic attendance and first adult clinic attendance. DMARD: disease-modifying antirheumatic drug.
We defined successful transfer as receipt of a letter from the first adult appointment, which did not occur in 14% of cases (n = 22), and receipt of a letter from the second adult appointment, which did not occur in 57% of cases (n = 87). Seven were currently being transferred and not included. Referral letter, health summaries, and copy letters were not documented as having been sent to the adult team from the pediatric team in 24% of cases (n = 36) or to patients themselves in 59% of cases (n = 89).
The results highlight the need for improved consistency of practice both within and between pediatric and adult rheumatology teams to ensure equity, quality, and successful outcomes of transitional care. The acknowledgment that transitional care is a team concern and not the role of a single staff member is fundamental to success10. The maintenance processes that will ensure informational continuity should be core knowledge for rheumatology training and staff induction programs. All such information should, in turn, be clearly defined in a written and agreed transition policy — a further core element of transition3,4,8.
The initial appointment in adult rheumatology for young people previously cared for in a pediatric center is crucial to ensure engagement in adult services and to establish a therapeutic relationship between the young person and their new rheumatology team. Success will be enhanced if significant lapses of care can be avoided and the adult service is adequately informed about the young person prior to the appointment. This is particularly important for young people taking DMARD/biologics, as well as for those with comorbidities.
Until the implementation of universal electronic patient records, the challenges of informational continuity between pediatric and adult rheumatology centers will remain. Such challenges are particularly pertinent to specialties such as rheumatology that transfer patients to multiple adult providers in geographically diverse hospitals (as opposed to a single regional clinic), often with incompatible information technology systems.
Although the responsibility for timely dictation of referral letters and summaries remains with clinical personnel, the collation of the paperwork, confirmation of what is sent and received, and the tracking of young people into adult care could be undertaken by adequately resourced administration staff in both pediatric and adult rheumatology teams. Such informational continuity will benefit patient care as well as much-needed longitudinal rheumatology research into young adulthood.








{kind=link}