Article Text

Abstract
Background SLE is an autoimmune disease that predominantly affects women. As most epidemiological and interventional studies are on populations with a clear female prevalence, the influence of gender in disease course, drug response and damage accrual is yet to be fully explored and comprehended.
Objectives To describe gender differences in disease course, comorbidities, use of medications and long-term outcomes of a large cohort of patients with SLE.
Methods Retrospective gender-based analysis of prospectively collected data from a monocentric cohort of Caucasian patients with SLE with at least 1 year of follow-up.
Results 417 patients were included, 51 men and 366 women. Men displayed a significantly higher median age at disease onset and diagnosis and a higher prevalence of late-onset SLE, serositis at disease onset, antiphospholipid syndrome (APS) and use of mycophenolate within the first year of disease. Women had a higher prevalence of haematological abnormalities, a higher cumulative exposure to azathioprine and higher cumulative dose of glucocorticoids at 5 years. Male patients had a shorter time to first damage item and a higher prevalence of damage at 1 and 5 years, but this association was no longer significant when late-onset patients were excluded. No differences were found in prevalence of childhood onset, delay between onset and diagnosis, time to renal involvement and histology, cumulative autoantibody positivity, number of flares and hospitalisations, median SLE Damage Index score, type of damage, age and time to first cardiovascular event, chronic kidney disease and death.
Conclusions In our cohort, clinical manifestations and disease course were similar in male and female patients; however, male patients displayed higher prevalence of APS and early damage accrual probably due to the later disease onset. These data highlight the importance of an intensive follow-up, prevention and treatment of complications in this category of patients, especially in the first years of disease.
- Lupus Erythematosus, Systemic
- Lupus Nephritis
- Autoantibodies
- Epidemiology
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available from the corresponding author, CT, upon reasonable request. The data are not publicly available due to their containing information that could compromise the privacy of research participants.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
In the past decades, many attempts have been made to identify distinguishing clinical characteristics in male patients with SLE, with controversial results.
Limitations of prior studies include small sample sizes, ethnic heterogeneity, variable follow-up duration or cross-sectional study design.
WHAT THIS STUDY ADDS
This is a cohort study on a large, ethnically homogeneous population with a long follow-up period. Clinical outcomes were evaluated at specific timepoints to reduce potential bias due to differences in follow-up duration.
In our cohort, clinical course was similar in men and women, but men were more prone to early damage, probably due to older age at disease onset in this group. There were no differences observed in the type of damage or comorbidities between genders, apart from antiphospholipid syndrome.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
These data can lay the foundation for identifying gender-specific strategies for the management of SLE.
Introduction
SLE is a complex autoimmune disease with a clear female prevalence and a special predilection for women of childbearing age.1
As male patients represent a minority in most epidemiological and interventional studies, gender-related issues, such as disease course and drug response, still need to be fully addressed. In the past decades, many attempts have been made to identify distinguishing clinical characteristics in male patients, with controversial results, which could be due to study biases (eg, small sample size, different ethnicities, variable duration of follow-up and disease duration) rather than real gender differences.2 In general, however, men seem to have the same disease spectrum as women but have a less favourable long-term outcome with higher risk of developing organ damage,3 especially in the first years of disease.
Our study was conducted to evaluate if Caucasian male patients with SLE have distinctive features at disease onset, over disease follow-up as well as in long-term outcomes.
Methods
This is a retrospective analysis of prospectively collected data from a monocentric cohort of patients with SLE. Patients were selected from the database of the lupus clinic of the rheumatology unit of the Azienda Ospedaliero-Universitaria of Pisa, Italy.
Patients
Patients of any age who met at least one internationally approved criteria for the classification of SLE,4–6 regularly followed up at our centre and with at least 1 year of follow-up were eligible for inclusion. Patients with <1 year of follow-up, incomplete clinical history or lack of seroimmunological parameters were excluded.
Data collection
The following demographic and clinical variables were collected from the database: date of birth, age, ethnicity, age at disease onset and diagnosis, delay between onset and diagnosis, disease duration, duration of follow-up, initial and cumulative manifestations, interval between disease onset and renal involvement, renal histology (at first biopsy), cumulative autoantibody positivity, smoking habit (ever) and presence of comorbidities (ie, hypertension, dyslipidaemia, chronic kidney disease (CKD), osteoporosis, diabetes mellitus, Sjögren’s syndromeSjögren’s syndrome (SS) and antiphospholipid syndrome (APS)).
Disease onset was defined as the first moment in which the patient fulfilled the classification criteria for SLE; disease duration was the interval between disease onset and last observation; follow-up time was the interval between the first visit and the last observation at our centre.
Age cut-offs for ‘late-onset’ and ‘childhood-onset’ SLE were >49 and <16 years, respectively.7 8
Disease manifestations were classified in (1) joint involvement, (2) mucocutaneous manifestations, (3) autoimmune cytopenias, (4) kidney manifestations, (5) neuropsychiatric SLE (NPSLE), (6) serositis, (7) systemic manifestations and (8) Raynaud’s phenomenon. Attribution to SLE was based on the physician’s clinical judgement.
Disease flares were defined using a modified SLE Flare Index9 (increase of at least 4 points in the SLE Disease Activity Index 200010 score between visits and/or new/worse disease manifestations); Physician’s Global Assessment was not considered. Flares were categorised as severe (SLE Disease Activity Index 12 or higher, new/worse NPSLE/vasculitis/myositis/platelets 60 000 or less/haemolytic anaemia/nephritis or hospitalisation for disease activity) or mild-moderate (less than 12) and were examined as a continuous variable (total number of flares) and as a dichotomous variable (presence or absence of flares) at 1, 5 and 10 years. Hospitalisations (defined as ‘hospitalisation for any cause ≥1 night’) were examined as a continuous variable (total number of hospitalisation) and as a dichotomous variable (presence or absence of hospitalisations) at 1, 5 and 10 years.
Cumulative exposure to oral and parenteral immunosuppressive drugs (azathioprine (AZA), mycophenolate mofetil (MMF) or mycophenolic acid, cyclosporine A (CyA), cyclophosphamide (CyC), rituximab (RTX), belimumab (BEL)) and cumulative dose of glucocorticoids (GCs) was estimated for each patient at 1, 5 and 10 years from disease onset.
Organ damage was assessed using the Systemic Lupus International Collaborating Clinics (SLICC)/American College of Rheumatology SLE Damage Index (SDI);11 SDI was calculated at 1, 5 and 10 years from disease onset. Damage was then analysed as a continuous (total damage score) and as a dichotomous variable (presence or absence of damage) at each predefined time point.
Based on the items of the SDI, we focused our analysis on six categories of damage: (1) renal damage; (2) disease-related damage (ie, renal damage, cognitive impairment, Jaccoud’s arthropathy, alopecia and splenectomy); (3) steroid toxicity (osteoporosis, diabetes, cataract and avascular necrosis); (4) premature ovarian failure (POF); (5) cancer (excluding dysplasia); and (6) cardiovascular (CV) events (myocardial infarction or stroke).
Age and disease duration at first damage item, at first CV event, at CKD and at death were also recorded. Cause of death was classified as (1) infection, (2) disease activity, (3) CV disease, (4) cancer and (5) unknown.
Statistical analysis
All the statistics were performed by using Stata V.15 or R V.4.2.2 packages for Mac.
Based on the result of the Shapiro-Wilk test for normality, continuous data were presented as mean and SD or median and IQR. For categorical variables, percentage in each category was displayed.
For categorical variables, data from male patients were compared with those from female subjects by using the χ2 test. Unpaired two-tailed t-tests or, for skewed data that do not reach the normal distribution after logarithm transformation, Mann-Whitney U tests, were used for continuous variables.
We estimated the causal effect of sex on SLICC at 1, 5 and 10 years using logistic regressions. When there was an effect, we used the R package MatchIt12 to estimate the effect of sex on damage while controlling for the following covariates: age at onset, disease duration and smoke. In this analysis, we have chosen the optimal full matching method, while the propensity score was estimated with probit regression. The quality of matches was assessed by using lower standardised mean differences and empirical cumulative distribution function statistics. Finally, we fit logistic regression models with SLICC as the outcome and the sex, covariates and their interaction as predictors and included the full matching weights in the estimation. Regression analysis was repeated excluding the late-onset group from the sample.
Results
A total of of 474 clinical records were reviewed, and 417 patients were included, 51 men (12.2%) and 366 women (87.8%); all patients were Caucasian.
The epidemiological characteristics of the whole cohort and of the two groups are summarised in table 1. Briefly, median age at onset (34 vs 26 years, p=0.0007) and diagnosis (41 vs 28, p<0.001), prevalence of late-onset SLE (19.6 vs 5.2%, p<0.0001) and smoking habit (48 vs 29.5%, p=0.004) were more common among men. No significant differences were found in childhood onset and median delay between onset and diagnosis.
Demographic characteristics of the whole cohort and of male and female patients
A significant difference was also observed in the median follow-up (4 years vs 7 years, p=0.006) and disease duration (10 years vs 17 years, p=0.001) between male and female patients.
Clinical characteristics and immunological parameters
In table 2, clinical characteristics of the disease at onset and during follow-up were summarised. At disease onset, men had a higher prevalence of serositis (15.7 vs 7.1%, p=0.037), while no difference was observed for the other clinical manifestations. During follow-up, a smaller proportion of men developed haematological manifestations (46 vs 66.9%, p=0.004), without other significant gender differences in clinical manifestations accrued. No differences were found in interval between disease onset and renal involvement (0 (0–5) vs 0 (0–3)) and the type of renal involvement at first biopsy. In addition, no differences were observed with respect to the prevalence of the different autoantibody specificities (see table 2).
Clinical manifestations, serological features and comorbidities
Comorbidities
As far as comorbidities are concerned, no differences in the proportion of patients with osteoporosis, hypertension, type 2 diabetes, CKD and dyslipidaemia were observed. Of the men with comorbidities, 5.6% were diagnosed with androgen deficiency.
Prevalence of APS was significantly higher in men (28.26% vs 15.7%, p=0.04), while no differences were observed in the association with SS (11.1% vs 6.6%, p=0.27).
Among the patients diagnosed with secondary APS, venous thrombosis was the most common manifestation in both sexes, occurring in 7 out of 12 men (58.3%) and 24 out of 57 women (49.1%). Arterial thrombosis occurred in 5 out of 12 men (34.7%) and in 16 out of 57 (28%) women, while the obstetric syndrome was present in 16 out of 57 women (28%). The type of involvement was unknown for four women. Comorbidities are summarised in table 2.
Therapeutic management
Overall, more women than men received at least one immunosuppressive drug (80.8% vs 72%), but the difference was not statistically significant.
Female patients received AZA more frequently than their male counterparts (38.61% vs 18% at last visit, p=0.004). At 1 year, MMF was administered in 29.17% men vs 15.4% women, (p=0.02).
Exposure to other traditional (including oral and intravenous CyC, AZA, CyA and MTX) and biological immunosuppressive drugs (ie, RTX and BEL) occurred at comparable frequencies at 1, 5 and 10 years.
Median cumulative GC dose at 5 years was significantly higher in women (8.55 (7–12) g vs 7 (4.5–8.5) g, p=0.0191). No differences were found in the proportion of patients GC-free at 5 years (27.66% men vs 36.49% women) and at last visit (27.66% vs 36.49%), median GC dose at last visit (4 (0–4) mg vs 2 (0–4) mg), median cumulative dose at 1 (2 (1.4–4.0) g vs 2 (1.4–4.5) g) and 10 years (14.9 (9.6–19) g vs 15.4 (11.4–20.8) g). A summary of the therapeutic management is provided in table 3.
Cumulative exposure to immunosuppressive drugs and GCs (6-methylprednisone)*
Relapses and hospitalisations
The proportions of patients with at least one flare at 5 years (35.71% in men vs 38.8% in women); severe flares ever (36.96% vs 40.57%); and total number of flares at 1, 5 and 10 years (median 1 (1–2) in both sexes) were similar in the two groups. Relapses and hospitalisations are summarised in table 4.
Cumulative* disease flares and hospitalisations
Damage
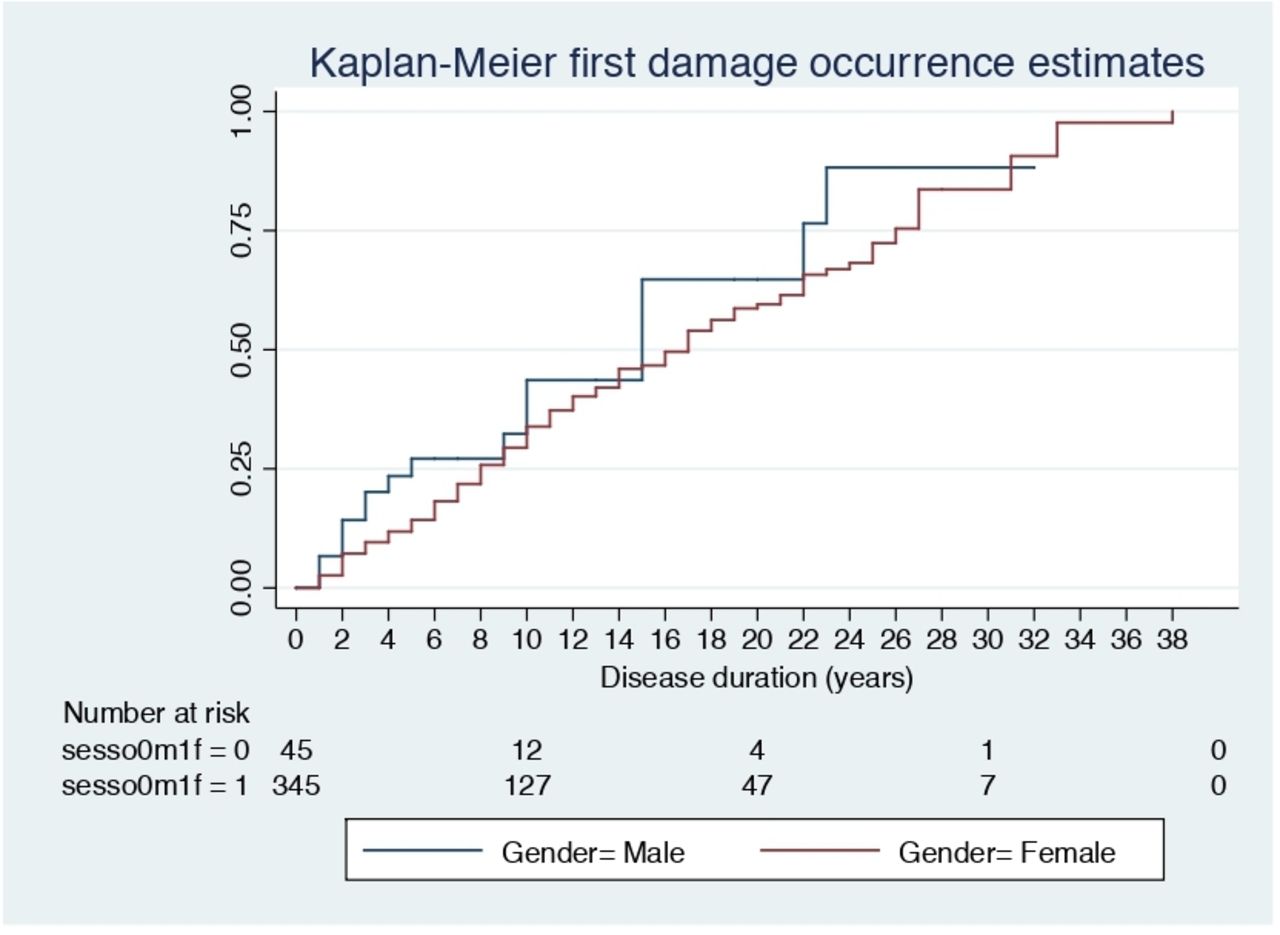
Age at first damage was significantly lower in women (40 (32–50) years vs 48 (43–3) years, p=0.01), but men had a shorter time to first damage (2 (0.5–9.5) years vs 8 (2–16) years, p=0.002) and a higher prevalence of damage at 1 year (20.83% vs 8.1%, p=0.005) and 5 years (34.37% vs 15.3, p=0.006). In the first logistic regression, the estimated effect of sex on damage was significant at both 1 (p=0.008) and 5 (p<0.0001) years. However, when we controlled for the covariates (age at onset, disease duration and smoke), the model only confirmed the effect at 5 years (p=0.032), while at 1 year, no effect was observed (p=0.204).
The proportion of patients with SDI >0 at 10 years, median total SDI at 1, 5 and 10 years, cumulative type of damage (ie, disease-related, renal, GC-related, CV and cancer), age and disease duration at first CV event and CKD, were similar in the two groups. Interestingly, 12.4% of female patients developed POF within the first decade of the disease.
Damage is summarised in table 5 and figure 1.
{kind=link}
Graph.
Cumulative* damage and mortality
Mortality
Of the 417 patients, 13 were lost at follow-up and their clinical outcome is unknown. Of the remaining patients of the total of 417 patients, 16 died (4 men and 12 women): 5 for cancer (1 pancreas, 1 colon, 1 melanoma, 1 lung and 1 lymphoma), 4 due to CV events (2 myocardial infarction, 1 aortic dissection and 1 sudden cardiac death), 4 due to infections (1 septic shock due to the combination of infected ulcers and aspiration pneumonia, 1 septic shock, 1 viral myocarditis and 1 COVID-19 pneumonia) and 2 due to disease complications (1 for renal impairment and 1 for mesenteric vasculitis). The cause of death was not available for one patient. Cause of death, disease duration (21 (16–27) in men vs 16 (7–27) in women) and age at death (54 (54–75) years vs 47 (35–60) years) did not differ significantly between the two groups.
Mortality is summarised in table 5.
Discussion
In our study, we assessed the presence of gender differences in clinical manifestations, autoantibody positivity, disease course, therapy and organ damage in a large monocentric cohort of Caucasian patients with SLE. As reported herein, we observed that the overall clinical expression of SLE was quite similar for both sexes, with no significant differences in major organ involvement and rate or severity of relapses. We also noted that, similar to previous observations, Caucasian men of our cohort had a higher prevalence of serositis,13–15 an older mean age at disease onset16 17 and a higher rate of smokers when compared with female counterparts.
Women had a higher prevalence of haematological abnormalities, higher cumulative exposure to AZA and higher cumulative dose of GCs at 5 years.
The higher use of AZA in women may be due to different needs related to gender: in women, indeed, disease onset usually occurs during childbearing age, and AZA is generally considered to be safe during pregnancy.
Univariate analysis also revealed that male sex was associated with greater damage accrual at 1 and 5 years, consistent with findings from large multiethnic inception cohorts such as Lupus in Minority Populations: NAture versus Nurture (LUMINA)17 and SLICC.18
However, unlike LUMINA,17 this study did not observe any significant difference in damage scores17 over the follow-up period. Generally speaking, damage accrual is influenced by genetic predisposition, age, lifestyle, comorbidities, disease severity and course, delay in diagnosis and treatment, type of organ involvement, GC use, adverse reactions to drugs and compliance of the patient.
In our cohort, the earlier damage accrual in men could be due to several factors, the first of which is older age at disease onset in men. Indeed, it is well known that in the general population, SDI items such as stroke, angina, myocardial infarction, valvular disease, renal impairment, cataracts, retinopathy, diabetes and malignancy are more common with increasing age. According to the results from the SLICC inception cohort,18 age has a non-linear effect on damage. Older patients may therefore have a greater sensitivity to inflammation and drug adverse effects due to reduced organ reserve.17
Another important possible contributor to early damage is smoking; indeed, in our cohort, there is a high frequency of smokers, especially among men.
Logistic regressions were performed to estimate the effect of sex on damage, controlling for age at onset, disease duration and smoking. The multivariate analysis confirmed that male sex is an independent predictor of damage at 5 years, but this association was no longer significant when late-onset patients were excluded. Therefore, the results suggest that age at disease onset is more strongly associated with damage than male sex in our cohort.
A lower median cumulative dose of GCs was also observed in men at 5 years; we could hypothesise that accelerated damage accrual could be due to less aggressive treatment approach. Interestingly, GC-related damage was similar in both groups.
Our results also did not confirm a higher risk of developing CKD17 19 20 and CV events17 19 20 in male patients. Interestingly, despite a higher prevalence of smokers among men, arterial CV events occurred at comparable rates, ages and disease durations in both sexes (see table 5), which is not the case for the general population.21 Noteworthy, women in the study had a significantly lower median age at their first CV event (46 (38–57) years) compared with the general population. According to the Italian National Institute of Health,22 the prevalence of acute myocardial infarction in the general adult population is 1.6% in men and 0.6% in women, while cerebrovascular accidents occur in 0.7% of patients, regardless of sex. Consistently with previous observations, in our cohort the prevalence of CV events was remarkably higher (11.76% in men and 8.81% in women). Systemic inflammation, indeed, promotes atherosclerosis and patients with SLE have an increased risk (9–50 folds) of developing CV events compared with the population of similar age without SLE, especially those aged 36–45 years.23–25
Also osteoporosis occurred at a similar rate in both sexes (17.4% vs 23.5%, p=0.6; male to female ratio 1:1.35), while in the general population, the ratio is 1:3.26 27 The aetiology of bone loss in SLE is multifactorial, including traditional osteoporosis risk factors (such as age and menopause), inflammation and drug-induced adverse effects.28 29
The high prevalence of osteoporosis in our male patients could be due to several factors: use of GCs, a well-known risk factor for secondary osteoporosis,30 older age at last visit, higher prevalence of smoking (50% of male patients with OP vs 26% of female patients), and a non-negligible presence of patients with androgen deficiency (5.6% of all men, 12% of those with OP).
Another interesting finding is that, unlike previous studies, we did not detect any difference in the presence of anti-dsDNA31 32 and other autoantibodies, including antiphospholipid (aPL) autoantibodies, between men and women.
Nevertheless, men had a higher rate of APS, suggesting that other factors, such as smoking, can play a crucial role in the pathogenesis of the syndrome in these cases.33 Indeed, in our cohort, 23 of 70 (32.85%) patients with APS were smokers (53.8% of men vs 20.1% of women). Additionally, men were older, and the role of atherosclerosis in arterial events cannot be excluded. Thus, the first limitation of this analysis relies on the fact that it is not easy to completely understand the real contribution of aPL to vascular events with respect to traditional CV risk factors.
Other limitations include the retrospective study design and the lack of information on the degree of patient’s adherence to the treatments, which may influence damage progression.
Moreover, due to the small subgroup of male patients, the possibility of committing a type II statistical error could not be excluded. Furthermore, this is an observational study in a tertiary referral centre for SLE, a limitation in the generalisability of the results cannot be excluded. Therefore, selection bias cannot be ignored. We tried to reduce the possible impact using a propensity analysis and repeating the elaboration after eliminating the late-onset group from the sample.
Our study has several strengths. Patients in our cohort have a homogeneous ethnic and geographical background. Moreover, the prospective collection of data, the long-term follow-up time and the completeness of the clinical data due to a good adherence to routine visits should be considered. Moreover, evaluation of clinical outcomes at 1, 5 and 10 years, permits limitation of potential bias due to a different disease duration and follow-up.
In conclusion, we have described a large Caucasian population focusing on sex and gender differences in disease course, therapy and damage. Our findings suggest that, in Caucasians, men and women have a more similar disease course than expected.
However, male patients displayed higher prevalence of APS and earlier damage accrual probably due to the later disease onset. These data highlight the importance of an intensive follow-up, prevention and treatment of complications in this category of patients, especially in the first years of disease.
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available from the corresponding author, CT, upon reasonable request. The data are not publicly available due to their containing information that could compromise the privacy of research participants.
Ethics statements
Patient consent for publication
Ethics approval
This study was reviewed and approved by local ethical review board ‘Comitato Etico Area Vasta Nord Ovest’, reference number 14478.
References
Footnotes
Contributors All the authors contributed to the data collection. FT wrote the article. CT, FT and MLM performed the statistical analysis. CT and MM reviewed the concept of the study and the article, MM is the guarantor of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.