Article Text

Abstract
Background Laboratory tests of blood and sometimes urine are used to diagnose and to monitor disease activity (DA) in SLE. Clinical practice would be simplified if non-invasive urine and salivary tests could be introduced as alternatives to blood samples. We therefore explored the levels of innate immunity-related biomarkers in matched serum, urine and saliva samples from patients with SLE.
Methods A total of 84 patients with SLE selected to represent high and low general DA, and 21 controls were included. All participants underwent a thorough clinical examination. General DA and renal DA were measured. The levels of colony-stimulating factor (CSF)-1, interleukin (IL)-34, tumour necrosis factor (TNF)-α, interferon-γ-induced protein (IP)-10, monocyte chemoattractant protein (MCP)-1, calprotectin, macrophage inflammatory protein (MIP)-1α and MIP-1β were analysed by immunoassays and related to DA.
Results CSF-1, TNF-α, IP-10 and MCP-1 in saliva, serum and urine, as well as calprotectin in saliva and urine were increased in patients with SLE as compared with controls (p<0.05). TNF-α, IP-10 and MCP-1 in saliva, serum and urine, and CSF-1 in saliva and serum distinguished patients with SLE from controls (area under the curve >0.659; p<0.05 for all). CSF-1 in serum and urine, and calprotectin in saliva and urine, as well as TNF- α, IP-10 and MCP-1 in urine correlated positively with measures of general DA (p<0.05). Patients with SLE with active renal disease presented elevated levels of TNF-α, IP-10 and MCP-1 in urine and CSF-1 and IP-10 in serum as compared with patients with SLE with non-active renal disease.
Conclusions Our investigation demonstrates that saliva is a novel alternative body fluid, with potential for surveillance of general DA in patients with SLE, but urine is more informative in patients with SLE with predominantly renal DA.
- autoimmunity
- systemic lupus erythematosus
- disease activity
Data availability statement
Data are available on reasonable request from the authors.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Saliva and urine are fluids with potential to detect biomarkers.
The potential of markers in saliva and urine to distinguish patients with SLE from controls, and to evaluate disease activity (DA) in SLE is however poorly explored.
What does this study add?
Patients with SLE have higher levels of colony-stimulating factor-1, tumour necrosis factor (TNF)-α, interferon-γ-induced protein (IP)-10 and monocyte chemoattractant protein (MCP)-1 in saliva, serum and urine, and patients with active renal disease have higher TNF-α, IP-10 and MCP-1 levels in urine.
Biomarkers in saliva, serum and urine correlate positively with SLE DA.
How might this impact on clinical practice or future developments?
Saliva and urine represent alternative body fluids for detection of biomarkers related to SLE DA.
Introduction
SLE is a chronic autoimmune disease characterised by activation of innate and adaptive immune responses that may lead to severe organ damage. The aetiology behind autoimmunity in SLE is still unclear however, innate immune responses in SLE are linked with defects in apoptotic clearance, break of tolerance and a type I interferon (IFN) signature.1 2 Type I IFNs are mainly produced by plasmacytoid dendritic cells, which are stimulated by immune complexes and neutrophil extracellular traps (NETs), produced during NETosis of neutrophils.2 3 A state of systemic inflammation is also present in SLE with high levels of pro-inflammatory cytokines such as tumour necrosis factor (TNF)-α, interleukin (IL)-6 and IFN-γ-induced protein (IP)-10.4 5
Monocytes and their migration and function in response to cytokines and chemokines are essential in inflammation. Colony-stimulating factor (CSF)-1 is the primary regulator of the survival, proliferation, differentiation and function of mononuclear phagocytes. Of note, CSF-1 also induces monocytes to produce high levels of several cytokines, for example, TNF-α,6 which stimulates IP-10 secretion,7 and both appear to be involved in the pathogenesis of SLE and correlate with renal involvement.4 8 In addition, CSF-1 has been described to predict lupus nephritis (LN).6 9 The monocyte chemoattractant protein (MCP)-1 is produced mainly by monocytes. Its function is, among others, to regulate the migration and infiltration of monocytes and its expression is also upregulated by TNF-α.10 11 Finally, the heterodimeric complex calprotectin (S100A8/A9) is a danger-associated molecular pattern molecule mainly produced by monocytes and neutrophils. Increased serum levels of S100A8/A9 have been observed in SLE.12
The clinical presentation of SLE is heterogenous and can affect multiple organs including skin, joints, mucosa, kidneys, nervous system and bone marrow. Both the extent of accrued damage and disease activity (DA) contribute to the severity of SLE, which varies from mild to severe and can sometimes lead to life-threathening complications.13 The involvement of the mouth and oral mucosa in SLE is evident and the presence of oral ulcers is included in all three major sets of criteria for classification of SLE.14–16 Dry mouth is another common oral manifestation, which is part of secondary Sjögren’s syndrome (SS).5
Potential biomarkers of DA may be present in other types of body fluids than serum/plasma. However, despite engagement of the oral cavity in SLE, analysis of cytokines in saliva as potential disease markers remains poorly explored. More studies are perfomed in urine, but to date these results have limited use in clinical pratice.17 To get a more complete picture, we explored the levels of innate immunity-related biomarkers in matched saliva, serum and urine samples from patients with SLE and population controls in relation to measurements of general and renal DA. Moreover, we evaluated their ability to discriminate patients with SLE from controls.
Our purpose was to investigate whether there are less-invasive options than blood samples to distinguish patients with SLE from controls and to evaluate DA in SLE. Our findings suggest that both saliva and urine are alternative body fluids where biomarkers associated with SLE and with DA in SLE can be measured.
Materials and methods
Study population and sample selection
Subjects for this study were selected from a cohort of 546 consecutive patients with SLE managed at the Unit of Rheumatology, Karolinska University Hospital Stockholm, Sweden. Patients with SLE were >18 years old and fulfilled four or more of the American College of Rheumatology (ACR) 1982 revised classification criteria for SLE.16 Controls were recruited through the national registration number in the Swedish national population registry, which includes date of birth and is coded for sex. We also used region of living for matching. The exclusion criterion for the controls was a diagnosis of SLE. Controls were matched for age, sex and region of living to the first 322 patients with SLE in the SLE cohort. All study subjects were investigated in person by a rheumatologist and a nurse. A thorough medical file review was performed and DA was estimated by two validated indices, the Systemic Lupus Activity Measure (SLAM)18 19 and SLE DA Index (SLEDAI-2K).20 Renal DA was defined according to the British Isles Lupus Assessment Group index as never present (BILAG score E), non-active (BILAG scores C and D) and active (BILAG scores A and B).21 Organ damage was assessed by Systemic Lupus International Collaborating Clinics/ACR Damage Index.22
Sufficient sample volume, 250 µL from each of matched serum, saliva and urine, to conduct the laboratory analysis was available from 333 of the 546 patients with SLE in our cohort. Patients with missing data from either the SLAM or the SLEDAI-2K indices were thereafter excluded, leaving a total number of 294 patients with SLE. Since we were interested in patients with high and low DA, patients were divided into three groups. One group with low DA (SLAM <7 and SLEDAI-2K <4; n=50) and one group with high DA (SLAM >7 and SLEDAI-2K >4; n=63) were identified. According to these definitions of low/high DA, the third group, 181 patients, was discordant for DA by SLAM and SLEDAI-2K, and this group was excluded. With the purpose of avoiding over-representation of a particular age in any of the groups, we selected 42 patients from the high and 42 patients from the low DA groups, and 21 controls with a relatively similar and normal distributed age for final inclusion, and we also included a similar number of gender representation in each group.
Sample collection
At inclusion, all participants were fasting for 12 hours before collection of blood, urine and saliva samples. The first morning urine was collected. The participants were asked to avoid tobacco consumption; brushing teeth and using lipstick 1 hour prior to saliva collection. Whole unstimulated saliva was collected by passive drooling during 15 min23 for assessment of SS according to the ACR/European League Against Rheumatism criteria,24 then placed on ice followed by centrifugation (335 g×10 min). The salivary flow (mL/min) was recorded. Serum, urine and saliva samples were stored at −70°C until analysis.
Serological investigations
ANAs were analysed by indirect immunofluorescence in Hep-2 cells (Immunoconcepts, Sacramento, California, USA). ANA subspecificities anti-dsDNA, anti-SSA-Ro52, anti-SSA-Ro60, anti-SSB-La, anti-Sm, anti-SmRNP, anti-RNP68, anti-RNPA, anticardiolipin IgG/M and anti-β2-glycoprotein1 IgG/M antibodies were analysed by multiplexed bead technology using BioPlex 2200 system (Bio-Rad Laboratories, Hercules, California, USA). Routine laboratory tests and analyses of complement factors and immunoglobulins were performed according to clinical routine at the Department of Clinical Chemistry at the Karolinska University Hospital Stockholm, Sweden.
Immunoassays
CSF-1, IL-34 and calprotectin levels were analysed by ELISA according to instructions provided by the manufacturer (R&D Systems, Minneapolis, Minnesota, USA). Readings were made in a microplate spectrophotometer (SpectraMAX 340, Molecular Devices, Sunnyvale, California, USA) with wavelength set to 450 nm and correction set to 540 nm. TNF-α, MCP-1, IP-10, macrophage inflammatory protein (MIP)-1α and MIP-1β were analysed using a bead-based multiplex immunoassay (Invitrogen, Carlsbad, California, USA) in a multiplex analyser (Bio-Plex 100, Bio-Rad Laboratories) according to manufacturer’s instructions. The determination of total amount of protein was assessed with Pierce BCA Protein Assay Kit (Thermo Fisher Scientific, Waltham, Massachusetts, USA). CSF-1, MCP-1 and calprotectin were detected in all samples in the three fluids. TNF-α was detected in 99%, 98% and 85% in saliva, serum and urine, respectively, while IP-10 was detected in 99%, 100% and 97%. IL-34 was detected in 91%, 60% and 52% of the saliva, serum and urine samples, respectively. MIP-1α was detected in 97% of the serum samples but only 30% of the saliva and urine samples. MIP-1β was detected in 95% of the serum samples and in 10% vs 25% of the saliva and urine samples, respectively. Markers with detectability <80% were not statistically evaluated.
Statistical analysis
Data analyses were performed using Statistical Package for Social Science, V.24 (IBM, Armonk, New York, USA) and JMP, V.13.0 (SAS Institute, Cary, North Carolina, USA). Continuous variables are presented as mean and SD or median and IQR, and categorical variables as frequencies. Group comparisons were performed using Student’s t-test, Kruskal-Wallis test, Mann-Whitney U test, Pearson’s χ2 test or Fisher’s exact test whenever appropriate. When multiple groups were compared, a Dunn-Bonferroni post hoc test was performed. Correlations between the biomarkers and with the clinical variables were determined by Spearman’s correlation coefficient, as well as the correlations between the fluids. Statistical significance was set at p ≤0.05 and rho ≥0.3, for comparisons and correlations, respectively. To evaluate the accuracy of the biomarkers to discriminate patients with SLE from controls, area under the receiver-operating characteristic curves (AUROC) and 95% CI were calculated for each marker.
Results
Clinical and laboratory characteristics of patients with SLE and controls
Basic clinical and laboratory characteristics of patients with SLE (n=84) and controls (n=21) are presented in table 1. There was no significant difference in age, gender or smoking history between the groups. Patients with SLE had lower P-albumin, and higher U-albumin levels, as well as lower levels of serum complement proteins C3, and C4. Patients with SLE had lower salivary flow compared with the controls. DA, as measured with the SLAM, was more commonly reported in the constitutional, the integument, the neuromotor, the joints and the laboratory domains. Twenty-two patients with SLE presented with oral ulcers (n=13 in the high DA and n=9 in the low DA group). Of the 21 controls included in this study, none had a diagnosis of primary SS, secondary (s)SS, nor tested positive to any of the SSA/SSB antibodies. Equally, there were no cases with kidney disease or any other inflammatory disease, and no controls were treated with immunosuppressants.
Clinical and laboratory characteristics of patients with SLE and controls
Inflammatory markers in saliva, serum and urine by general DA in SLE
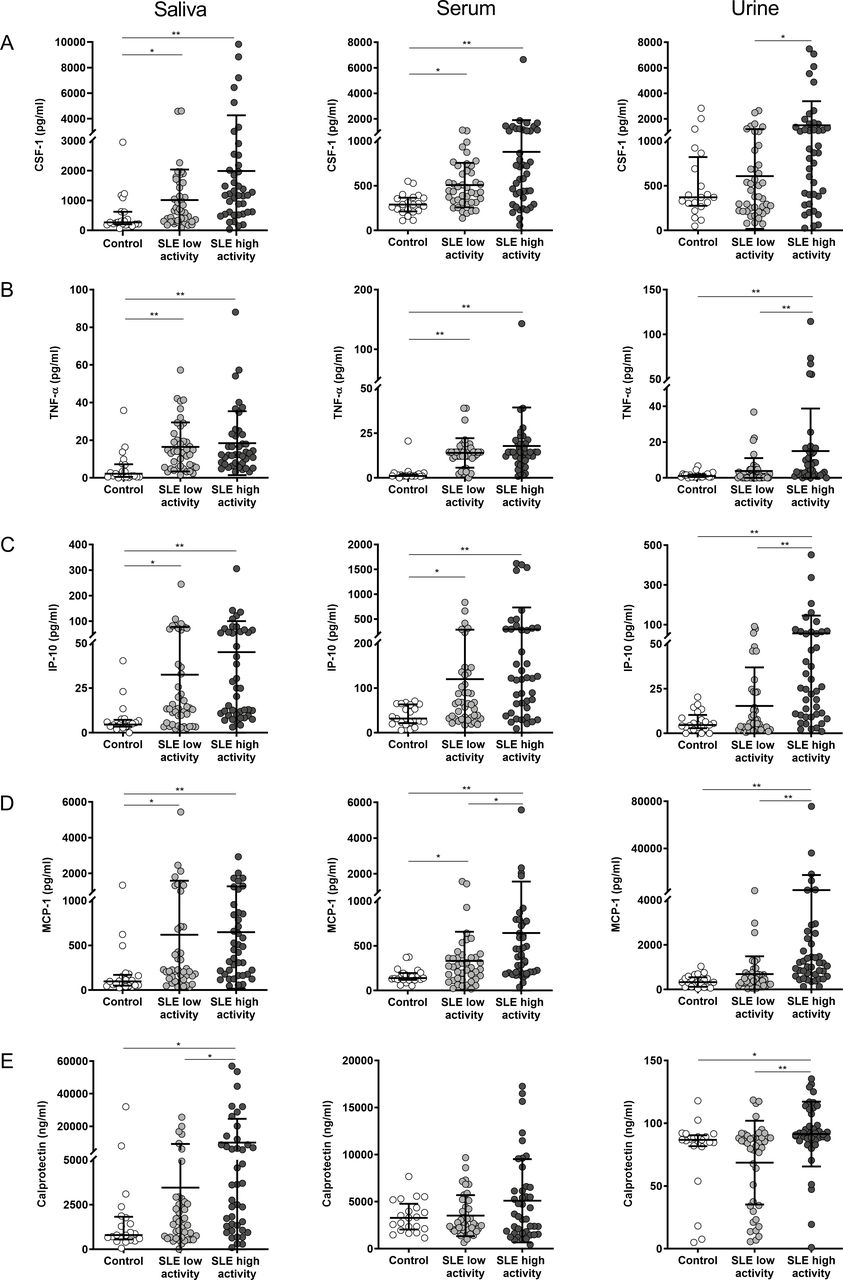
CSF-1 levels in saliva and serum were higher in patients with SLE with both low and high DA, as compared with the controls. Furthermore, patients with SLE with high DA compared with low DA presented higher CSF-1 levels in urine (figure 1A). The levels of TNF-α and IP-10 in saliva and serum were higher in patients with SLE in both the low and the high DA groups compared with controls. Higher TNF-α and IP-10 were also found in urine from patients with SLE with high DA compared with both low DA and controls (figure 1B and C). Salivary and serum levels of MCP-1 were higher in patients with SLE of both low and high DA groups compared with controls. Higher MCP-1 levels were also measured in serum from patients with SLE with high DA compared with patients with low DA. In urine, MCP-1 levels were higher in patients with SLE with high DA in comparison with the low DA group and controls (figure 1D). Similarly, higher levels of calprotectin in saliva and urine were found in patients with SLE with high DA compared with both low DA and controls. No difference was found in serum calprotectin levels between groups (figure 1E).
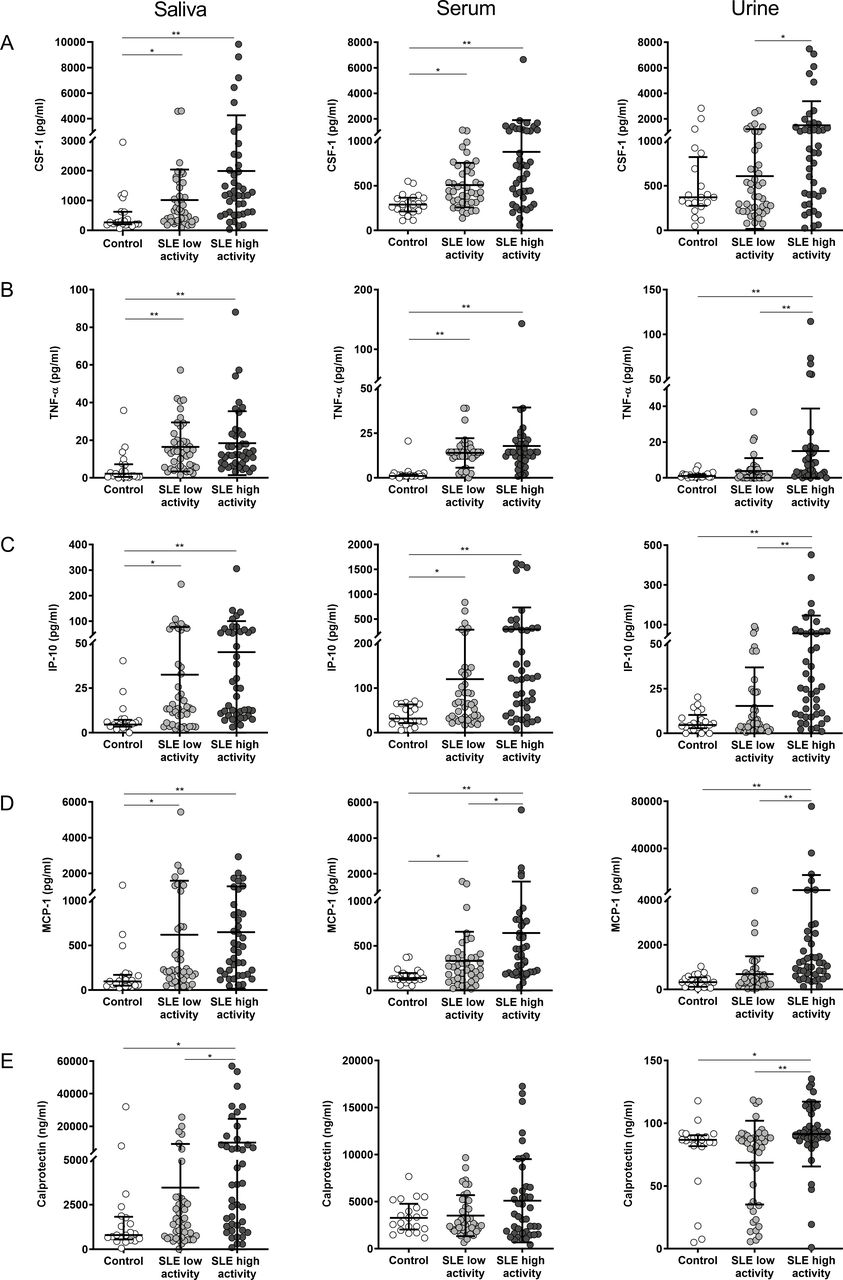
Inflammatory markers in saliva, serum and urine from patients with SLE and non-SLE controls. Levels of colony-stimulating factor (CSF)-1 (A), tumour necrosis factor (TNF)-α (B), interferon-γ-induced protein (IP)-10 (C), monocyte chemoattractant protein (MCP)-1 (D) and calprotectin (E) in saliva, serum and urine from controls (n=21) and patients with low SLE disease activity (n=42) and high SLE disease activity (n=42). *P<0.05, **p<0.01 (Kruskal-Wallis with Dunn-Bonferroni post hoc test).
Levels of IL-34 in saliva did not differ significantly between groups. MIP-1α showed higher levels in serum of the low and high DA, as compared with the controls. Also, MIP-1β in serum showed increased levels in both the controls and the high DA group as compared with the low DA group (online supplemental figure 1). Cytokines in saliva did not differ between patients with SLE with as compared with without oral ulcers (data not shown). Results were not altered when we adjusted the salivary cytokine levels for salivary flow.
Supplemental material
Inflammatory markers in saliva, serum and urine by renal DA in SLE
In serum, patients with SLE with active renal disease (here defined by BILAG A and B) had increased levels of CSF-1 and IP-10 as compared with non-active renal disease (BILAG C and D), and increased CSF-1 levels as compared with patients who had never had renal disease (BILAG score E) (figure 2A,C). In urine, the levels of TNF-α, IP-10 and MCP-1 were higher in patients with SLE with active renal disease as compared with the non-active group, and increased TNF-α and IP-10 levels were found in the active renal group as compared with the group with no previous renal disease (figure 2B–D). No significant differences between groups were found in the levels of Calprotectin (figure 2E), nor in any of the measured markers in saliva in relation to renal DA. The results were not affected when we adjusted the salivary cytokine levels for salivary flow.

Inflammatory markers in saliva, serum and urine from patients with SLE according to renal disease activity. Levels of colony-stimulating factor (CSF)-1 (A), tumour necrosis factor (TNF)-α (B), interferon-γ-induced protein (IP)-10 (C), monocyte chemoattractant protein (MCP)-1 (D) and calprotectin (E) in saliva, serum and urine from patients without kidney involvement (n=46) and those with non-active (n=25) and active renal disease (n=12). Data were missing for one patient. *P<0.05, **p<0.01, ***p<0.001 (Kruskal-Wallis with Dunn-Bonferroni post hoc test).
Correlations of inflammatory markers in saliva, serum and urine with clinical variables in SLE
Correlations between the markers in saliva, serum and urine with age, disease duration and DA, as measured by SLEDAI and SLAM, are presented in figure 3. In saliva, CSF-1, TNF-α and MCP-1 levels correlated positively with age. Salivary TNF-α correlated with disease duration and calprotectin to both DA indices. In serum, CSF-1 was positively correlated with disease duration and DA. In urine, all the included markers correlated positively with SLEDAI and SLAM.

Correlation heat map of clinical characteristics and levels of inflammatory markers in saliva, serum and urine. Correlation heat map of clinical characteristics and colony-stimulating factor (CSF)-1, tumor necrosis factor (TNF)-α, interferon-γ-induced protein (IP)-10, monocyte chemoattractant protein (MCP)-1 and calprotectin levels. Spearman’s correlation was used. *P<0.05, **p<0.01.
Correlations between inflammatory markers in saliva, serum and urine
Correlations between the analysed markers within saliva, serum or urine, and correlations between the fluids for each of the markers are presented in online supplemental figure 2. In brief, all the markers in saliva, except TNF-α and calprotectin, correlated with each other. In serum, CSF-1, TNF-α, IP-10 and MCP-1 correlated with each other. All the markers in urine correlated with each other. CSF-1 in saliva correlated with MCP-1 and IP-10 in serum. Salivary TNF-α correlated with CSF-1, IP-10 and MCP-1 in serum. MCP-1 in saliva correlated with its counterpart in serum. Salivary IP-10 correlated with its counterpart and with MCP-1 in serum. CSF-1 in serum correlated with IP-10 and MCP-1 in urine. MCP-1 in serum correlated with IP-10 in urine. IP-10 in serum correlated with calprotectin in urine. TNF-α in serum correlated with MCP-1 in urine. MCP-1 and IP-10 in urine correlated with its counterpart in serum.
Supplemental material
Ability of inflammatory markers in saliva, serum and urine to discriminate SLE
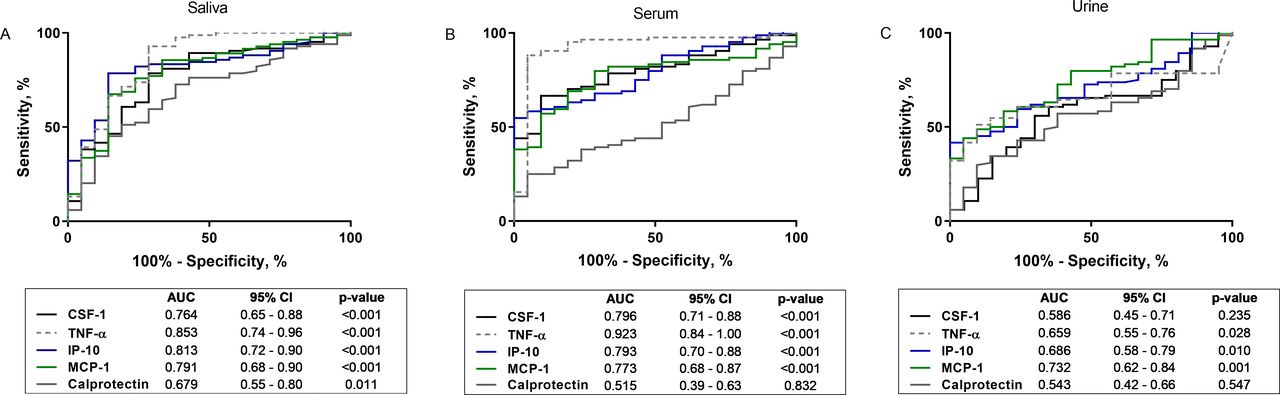
Given the observed difference in the levels of several of the analysed proteins in saliva, serum or urine, their abilities to differentiate patients with SLE from controls were assessed. Receiver operating characteristic (ROC) curve analysis showed that calprotectin levels in saliva along with CSF-1, TNF-α, IP-10 and MCP-1 in both saliva and in serum were capable to distinguish patients with SLE from controls. In particular TNF-α in serum had a high discriminatory power (ROC AUC 0.92) (figure 4A,B). In urine, TNF-α, IP-10 and MCP-1 levels also showed potential to discriminate between SLE and controls (figure 4C).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Potential of inflammatory markers in saliva, serum and urine to reflect SLE. Area under the curves (AUC) and 95% CI to assess the ability of colony-stimulating factor (CSF)-1, tumor necrosis factor (TNF)-α, interferon-γ-induced protein (IP)-10, monocyte chemoattractant protein (MCP)-1 and calprotectin in saliva, serum and urine to differentiate SLE from healthy participants.
Discussion
To the best of our knowledge, this is the first study analysing potential markers related to innate immunity in patients with SLE and controls in the three matched body fluids, saliva, serum and urine. Our main findings are elevated levels of CSF-1, TNF-α, IP-10 and MCP-1 in saliva and serum of patients with SLE compared with controls. Furthermore, we observed elevated levels of TNF-α, IP-10 and MCP-1 in urine from patients with SLE with active renal disease as compared with those with non-active renal disease.
In our study, TNF-α, MCP-1 and IP-10 were elevated in patients with SLE as compared with controls in saliva and serum, but only serum MCP-1 levels differed between the high and low DA groups. Furthermore, the levels of TNF-α, MCP-1 and IP-10 in urine also differed significantly between the high and low DA groups. High serum levels of TNF-α, and MCP-1 and IP-10, were in a previous study from our centre associated with higher general DA.4 These findings are also in line with previous reports of increased serum levels of TNF-α and MCP-1 as well as IP-10, with correlations to DA in patients with SLE.25 26
We used renal BILAG as measure of renal DA. Urinary TNF-α, IP-10 and MCP-1 levels, as compared with the other fluids, stand out for their positive associations with renal DA. These findings are in line with the study by Abujam et al, who demonstrated that MCP-1 and IP-10 in urine outperforms serum with regard to renal activity, and furthermore they reported declining levels in response to treatment.27 Of importance, we also found that many of the investigated markers in urine presented strong correlations with both general and renal DA. This is in line with previous reports showing a positive correlation of urinary MCP-1 with DA,28 and studies demonstrating correlations between the urinary levels of MCP-1 and IP-10 with active renal involvement.8 27 29–31
Our results confirm the simultaneous presence and correlation between TNF-α, IP-10 and MCP-1 in urine as well as serum and saliva. Although it is not clear whether their simultaneous presence is a result of a co-dependent upregulation, these chemokines/cytokines are all involved in the early phases of several autoimmune diseases.32 33 T helper (Th)-1 lymphocytes are responsible for enhanced production of TNF-α and IFN-γ, both of which induce IP-10 secretion from a variety of cells, creating an amplification feedback loop and perpetuating the autoimmune process, which shifts towards Th-2 immunity over the first years from diagnosis, resulting in raised MCP-1 and declining IP-10 concentrations.7 In our study, we did not perform repeated measures of these chemokines, and we believe that more studies following the levels of these chemokines longitudinally in patients with SLE are needed.
CSF-1 is the major haematopoietic growth factor for macrophages, and it has previously been implicated in SLE.9 In similarity to TNF-α, MCP-1 and IP-10, we observed increased levels of CSF-1 in saliva and serum of patients with SLE with both high and low DA as compared with controls. We also found elevated levels of CSF-1 in serum from patients with SLE with active compared with non-active renal DA, although this observation was not confirmed in urine. Our results are consistent with the findings by Menke et al, who elaborately studied CSF-1 levels in serum and urine, both in murine and human SLE.34 In a follow-up study, correlations were found between serum/urine levels and histological LN activity and declining serum/urine levels were associated with good treatment response.9 Both Menke et al and Tian et al also propose that urinary levels of CSF-1 precede and predict renal flares.35 Elevated CSF-1 in saliva is a novel finding in SLE, although our group has previously studied levels of CSF-1 in saliva from the general population and demonstrated increased levels related to age, smoking and general complaints such as muscle pain and local oral conditions, for example, periodontitis and caries.36 In accordance, we also noted a correlation between CSF-1 levels in saliva with age in the current study.
We report higher levels of calprotectin, a heterodimer of S100A8 and S100A9, which is mainly a marker of neutrophil activation, in saliva and urine from patients with SLE with high and low general DA as compared with the controls. Calprotectin has been implicated in local organ damage in SLE. Lood et al demonstrated an upregulation of calprotectin associated with type I IFN and cardiovascular diseases, especially myocardial infarction.12 37 Elevated calprotectin in serum and on the surfaces of immune cells in patients have also been reported previously.37–39 Donohue et al reported increased urinary levels of calprotectin in patients with juvenile-onset SLE with active LN.40 However, in our study, we could not confirm these findings. A possible reason might be the difference between juvenile onset in their study group, and the later disease onset, 34 years, in our cohort. Age at disease onset is one of several factors which are known to be associated with differences in the clinical features and disease phenotypes.41 42 A previous investigation from our group has shown elevated salivary calprotectin levels in patients with inflammatory bowel disease.43 In our study, we did not find statistically significant differences in the serum levels of calprotectin between the groups, which might be explained by the sample size included. Interestingly, proteomic analysis of saliva from patients with SLE identified the homodimer S100A8 to be almost four times higher as compared with controls.44
It is noteworthy to mention that the differences found with regard to DA might reflect the close relationship between active LN and a high general DA score, since renal activity is highly weighted in the DA indices, especially in the SLEDAI-2K.19 21 45 We found enhanced levels of the analysed markers in saliva in patients with high general DA, but not in patients with predominantly renal DA where urine was more informative. A possible explanation of these results may be that local production of cytokines/chemokines, such as IP-10, in inflamed organs is responsible for the recruitment of mononuclear cells and local organ damage, as it has been shown in several types of cutaneous damages in SLE.46 The cellular sources and possible local production of the included markers in this study deserve further investigation.
The ability of the studied biomarkers to discriminate patients with SLE from controls was also assessed. AUROC analysis was performed. Especially TNF-α was a good discriminator of patients with SLE from controls with AUROC of 0.92 in serum. Notably, it also performed remarkably well in saliva, with an AUROC of 0.85. CSF-1, TNF-α, IP-10 and MCP-1 in both saliva and serum also showed potential to distinguish patients with SLE from controls, all with AUROC >0.7. These observations are supported by previous reports of TNF-α and CSF-1 in circulation and in urine.4 9 In urine, MCP-1 had the best ability to separate patients with SLE from controls, which is in line with previous findings of MCP-1 as a urinary biomarker for LN,28 47 however IP-10 and TNF-α also performed fairly well in urine. Taken together, the analysed markers have to a varying extent, depending on fluid, the ability to discriminate patients with SLE from controls and active from inactive SLE, suggesting that both saliva and urine are potential alternatives to serum when diagnosing SLE and monitoring general SLE and renal DA.
Strengths and novelties of this study include the analyses of inflammatory biomarkers in three different matched fluids serum, urine and saliva, as well as the the selection of samples from a large and well-characterised SLE cohort with matched population controls. We specifically chose patients with high and low DA as confirmed by two independent activity indices; thus, the majority of patients with intermediate or discordant DA according to SLAM and SLEDAI-2K were not investigated. Few studies have previously investigated possible biomarkers in saliva of patients with SLE. Local salivary gland infiltration of leucocytes, which is well known in SS, a common condition secondary to SLE,5 are presumably responsible for the degradation of the salivary glands and they could be a possible explanation to our findings in saliva. However, we selected the patients with SLE by availability of saliva, which represents a weakness and it is likely that we excluded an important subgroup of patients with SLE with sSS, where low or loss of salivation is an important characteristic. Given that our results show differences in saliva for SLE in general, it is possible that the salivary results would have been even more evident in patients with sSS. Future studies with simultaneous salivary glands biopsies are needed to investigate whether salivary levels reflect degradation or inflammation in the salivary glands. Only few patients presented with oral ulcers, thus further studies are needed to elucidate how ulcers influence salivary measurements. It is also possible that different collection methods have an impact on cytokine measurements.48
It is worth mentioning that the levels of pro-inflammatory cytokines in saliva, such as CSF-1 and TNF-α, might also be affected by the presence of periodontitis.49–51
In this study, we did not investigate the oral status, but this is an important aspect for further studies. Although not all the available patient samples were used, the number of patients remaining untested was low and differed between the high/low DA groups, we therefore considered them not useful for reproducibility testing. Future studies including assessment of SLE treatment-naïve patients, larger cohorts and longitudinal follow-up will also be important to evaluate these markers at disease onset and to further validate our findings.
Our investigation demonstrates that CSF-1, TNF-α, IP-10 and MCP-1 in saliva and/or urine provide ability to distinguish patients with SLE from controls, and that they also reflect general DA. These observations are novel with regard to saliva. Furthermore, patients with SLE with active renal disease present elevated TNF-α, IP-10 and MCP-1 levels in urine. These are promising results suggesting that saliva and urine are potential non-interventional alternatives to serum when diagnosing and monitoring patients with SLE.
Data availability statement
Data are available on reasonable request from the authors.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by The Regional Ethical Review Board in Stockholm, Sweden 03-556 (031216). Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors ES, EAB conceived and designed the experiments, and were guarantors of the study. GR and RL-J performed laboratory analysis. GR, RL-J, IG, ES, EAB analysed and interpreted the data. IG and ES recruited research subjects for the study. GR, RL-J, IG, ES, EAB wrote and edited the manuscript.
Funding This study was supported by grants from the Swedish Research Council (grant nos. 2012-02480, 2012-07110, 2014-33867), the Center for Innovative Medicine (CIMED, grant no. FoUI-954540) and Region Stockholm (EAB has a clinical researcher position grant no. FoUI-954341), Swedish Heart-Lung Foundation (grant nos. 20130430, 20130552, 20170257), Stockholm County Council (SOF funds and ALF, grant nos. 2014016, 20170038), The Swedish Society of Medicine, Ingegerd Johansson’s Foundation (SLS-713911), The King Gustaf V 80th Birthday Fund (grant no. FAI-2017-0390), The Swedish Rheumatism Association (grant no. R-739631), Karolinska Institutet’s Foundations, The Swedish Dental Society, clinical research grants from Sörmland county (no: DLL-614351, DLL-648991) and Folktandvården Stockholms Län AB, Sweden.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.