Article Text

Abstract
Objective Multiple guidelines recommend continuing hydroxychloroquine (HCQ) for SLE during pregnancy based on observational data. The goal of this individual patient data meta-analysis was to identify the potential benefits and harms of HCQ use within lupus pregnancies.
Methods Eligible studies included prospectively collected pregnancies in women with lupus. After a systematic literature search, seven datasets meeting inclusion criteria were obtained. Pregnancy outcomes and lupus activity were compared for pregnancies with a visit in the first trimester in women who did or did not take HCQ throughout pregnancy. Birth defects were not systematically collected. This analysis was conducted in each dataset, and results were aggregated to provide a pooled OR.
Results Seven cohorts provided 938 pregnancies in 804 women. After selecting one pregnancy per patient with a first trimester visit, 668 pregnancies were included; 63% took HCQ throughout pregnancy. Compared with pregnancies without HCQ, those with HCQ had lower odds of highly active lupus, but did not have different odds of fetal loss, preterm delivery or pre-eclampsia. Among women with low lupus activity, HCQ reduced the odds of preterm delivery.
Conclusions This large study of prospectively-collected lupus pregnancies demonstrates a decrease in lupus activity among woman who continue HCQ through pregnancy and no harm to pregnancy outcomes. Like all studies of HCQ in lupus pregnancy, this study is confounded by indication and non-adherence. As this study confirms the safety of HCQ and diminished SLE activity with use, it is consistent with current recommendations to continue HCQ throughout pregnancy.
- Lupus Erythematosus, Systemic
- Health services research
- Epidemiology
Data availability statement
Data are available on reasonable request from the principal investigators of each study.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Multiple international guidelines recommend prescribing hydroxychloroquine to women with SLE throughout pregnancy.
What does this study add?
Women with SLE taking hydroxychloroquine during pregnancy had lower disease activity, but did not have improved pregnancy outcomes.
This study demonstrated the limitations of observational data in studying the impact of medications on pregnancy outcomes, including bias by indication and limited data on adherence.
How might this impact on clinical practice or future developments?
To determine optimal treatments for SLE pregnancy, randomised and/or pragmatic trials will be essential to obtain reliable results to guide evidence-based care.
Given the limited harm and the potential benefit on SLE activity, this study supports existing guidelines that women with SLE should continue HCQ throughout pregnancy.
Introduction
The guidelines surrounding medication use to treat SLE (lupus) during pregnancy have largely been based on relatively small, university-based, retrospective or prospective cohort studies. Outside of pregnancy, hydroxychloroquine (HCQ) has been demonstrated to decrease lupus flares, risk of lupus nephritis (LN), renal damage from LN and death.1 2 HCQ has been prescribed by rheumatologists with expertise in lupus and pregnancy since the early 1990s, initially based on several small patient series and one small randomised trial showing higher rates of lupus activity and pregnancy complications in the 10 women randomised to stop or not take the drug compared with the 10 who took it throughout pregnancy.3–6 Analyses of retrospective and prospective lupus pregnancy cohorts also demonstrate some benefits, though generally not as dramatic as in this randomised study. The clearest signal has come from the Hopkins Lupus Cohort, in which women who stopped the drug for pregnancy had significantly higher rates of SLE flare, though not increased rates of pregnancy loss or preterm delivery.7 8 A recent meta-analysis of published observational studies of HCQ suggested a decrease in pre-eclampsia and gestational hypertension.9 Early data demonstrated no increase in congenital anomalies in infants with in utero HCQ exposure for malaria and more recent studies have confirmed this finding.10–12 A recent comparison of pregnancies in the USA with and without a filled HCQ prescription in the first trimester found a small but statistically significant increase in malformations, though two similar studies in Denmark and Canada did not find an increase in birth defects.13–15 The prescription of HCQ to manage SLE during pregnancy has been adopted as the standard of care in recent years, with multiple national and international rheumatology guideline groups recommending it for all women with lupus.16–19
We hypothesised that prior studies were underpowered to identify improvements in pregnancy outcomes related to HCQ. Therefore, we sought to combine the datasets from multiple prospectively collected lupus pregnancy cohorts to enhance our ability to identify the benefits or risks of HCQ therapy for lupus in pregnancy. Because of the small size of these cohorts, most publications did not present outcomes based on HCQ use, so a traditional meta-analysis based on published ORs was not possible. Instead, we completed an independent patient data (IPD) meta-analysis, collecting the datasets from each cohort, reanalysing each cohort in a similar manner, then combining each cohort’s results into a meta-analysis.
Methods
The meta-analysis was performed in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.20 The protocol was registered in September 2015 (25938 PROSPERO). The meta-analysis was approved by the Duke University Institutional Review Board (IRB no: Pro00066961).
Literature search strategy
The original literature search was conducted by a librarian and included Medline (via PubMed), Embase, the Cochrane Database of Systematic Reviews and Web of Science’s Core Collection (see online supplemental table 1). Search terms covered multiple forms of lupus and terms for pregnancies published after 2000. The search identified 2811 potential manuscripts and conference abstracts (figure 1).
Supplemental material

Flow diagram of search to identify eligible cohorts. IPD, independent patient data; PI, Principal Investigator.
Cohort inclusion and exclusion criteria
Only prospectively collected cohorts were included to avoid the bias of retrospective assignment of lupus activity (box 1). Cohorts with at least 25 lupus pregnancies delivered between 1995 and 2015 were included. Each investigator provided assurance that all women completed informed consent prior to enrolment in their cohort study, either prior to conception or prior to the completion of the pregnancy. Pregnant women with SLE were enrolled sequentially within each cohort from the rheumatology clinic and followed according to local care patterns. All cohorts included prospective data collection with documentation into the medical notes and/or a research database of real-time data about medication use and lupus activity. Minimal data were required for inclusion to ensure a broad range of datasets. All studies had to include variables assessing SLE and antiphospholipid syndrome (APS) diagnosis, lupus activity, pregnancy loss and lupus-related medications. To participate, the cohort investigator had to enter into a Data Use Agreement with Duke University.
Inclusion criteria for cohorts in the individual patient data meta-analysis
Cohort study parameters
Prospective pregnancy data collection
Women diagnosed with SLE according to a standard set of criteria
Women in the study signed informed consent for participation through an institutional review board-approved protocol
Features of the cohort dataset
Includes an assessment of lupus activity
Includes medications used to treat lupus during pregnancy
Includes information about pregnancy outcomes
Features of the publication
Manuscripts published between 2000 and 2015
Abstracts published between 2012 and 2015 at the ACR or EULAR Scientific Meetings
The cohort includes at least 25 pregnancies in women with lupus
Manuscript published in English
Data access for the studies included in the individual patient data meta-analysis
A member of the original research team is able to provide the clinical data and is willing to discuss the specific measures and data fields within cohort with the meta-analysis team.
A member of the original research team is willing and able to sign the Data Use Agreement and provide data to Duke University.
Analysis
Individual participant analysis: The exposure of interest was HCQ use during pregnancy, which included women who continued HCQ throughout or started in the first trimester and continued through pregnancy. Women who started HCQ in the second or third trimesters or who stopped HCQ during pregnancy were considered ‘unexposed.’ Outcomes of interest were analysed separately and included fetal loss (at any point during pregnancy), preterm delivery (<37 weeks’ gestation), early preterm delivery (<34 weeks’ gestation), pre-eclampsia and high disease activity during pregnancy. As a sensitivity analysis for the outcome of fetal loss, we excluded any losses that occurred prior to 10 weeks. Twin pregnancies were not included in analyses for the outcomes of preterm delivery, early preterm delivery and pre-eclampsia.
Lupus activity during pregnancy was assessed using different methods in the cohorts. For this meta-analysis, high disease activity was defined as physician global assessment (PGA) >1, SLE Disease Activity Index (SLEDAI) >4 at any point during pregnancy or flare per the treating rheumatologist, depending on the data available. PGA is on a scale from 0 to 3, with 0 indicating no lupus activity and 3 indicating severe lupus activity. SLEDAI is a weighted score that attributes varying levels of points to different disease manifestations.21 A variation for pregnancy, the SLEPDAI, was used in some cohorts.22 To facilitate the analysis, we generated new variables in each dataset to identify the disease activity, medications and pregnancy outcomes in a semiuniform fashion.
All prospective pregnancy cohorts are limited in their ability to collect early pregnancy losses that occur prior to study enrolment. The risk of pregnancy loss decreases with each passing week of gestation, so late enrolment artificially decreases the frequency of pregnancy loss. To limit for this bias, we only included women who were enrolled in their first trimester, prior to gestational week 14.
Each cohort was analysed separately, and then the ORs for each outcome of interest were combined to determine the overall association of HCQ treatment on pregnancy outcomes. Due to some women having multiple pregnancies within the same cohort, we randomly selected one pregnancy per woman to be included in the analysis. This corrected for any correlation between pregnancy outcomes within a patient. As a sensitivity analysis, we generated a second sample of one randomly selected pregnancy per patient; results were consistent with this sample.
Missing data: Data for the outcome of pre-eclampsia were missing for 45 pregnancies across cohorts, most from the Hopkins cohort (93%). Women who were missing data on pre-eclampsia were older (32 years vs 30 years), less likely to be using prednisone (27% vs 64%) and more likely to be using HCQ (84% vs 61%). There were no differences in disease duration, disease activity, azathioprine or LN history. To determine the effect of missing outcomes data on our results, we performed a series of single imputations assuming: (1) all missing data had pre-eclampsia and (2) all missing data did not have pre-eclampsia.
We performed meta-analysis summaries using a DerSimonian-Laird random-effects model and conservatively used the Knapp-Hartung approach to adjust the SEs of the estimated model coefficients.23 24 Binary outcomes were pooled as an OR with 95% CI which indicates no statistically significant effect when overlapping one. The meta-analyses were performed in R (V.3.5.3) using the “metafor” package (V.2.0-0).25 26
Heterogeneity of treatment effect
Due to the effects of lupus disease severity and manifestations on pregnancy outcomes, the results were estimated for the overall effect, as well as stratified by history of LN, APS and disease activity in the first trimester as recorded within each dataset. As we did not have data available on prepregnancy disease activity, we addressed bias by indication by presenting results for patients with LN, based on the assumption that HCQ prescription would be the standard of care for a patient with a history of or active LN during pregnancy.
Confounders
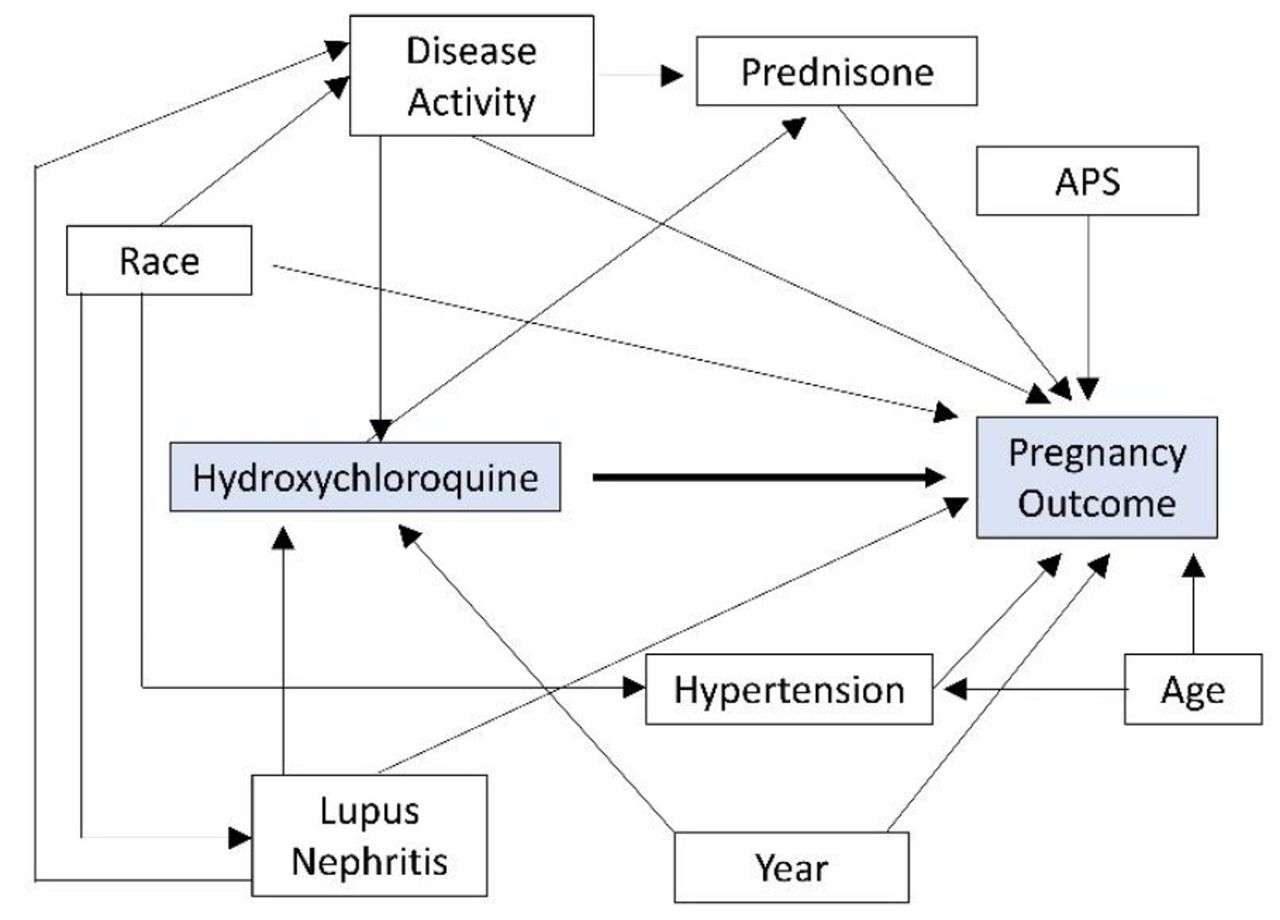
Based on a directed acyclic graph (figure 2), the minimal sufficient adjustment set for the association of HCQ use and pregnancy outcomes includes history of LN, disease activity and year of pregnancy. To account for these confounders, we present results stratified by history of LN, as well as disease activity in the first trimester. As we are restricting our analysis to pregnancies since 1995, we have not included year in our model. We did not adjust for prednisone use because it is a causal intermediate between HCQ and pregnancy outcomes and not a confounder; adjusting for prednisone would bias the effect estimate.
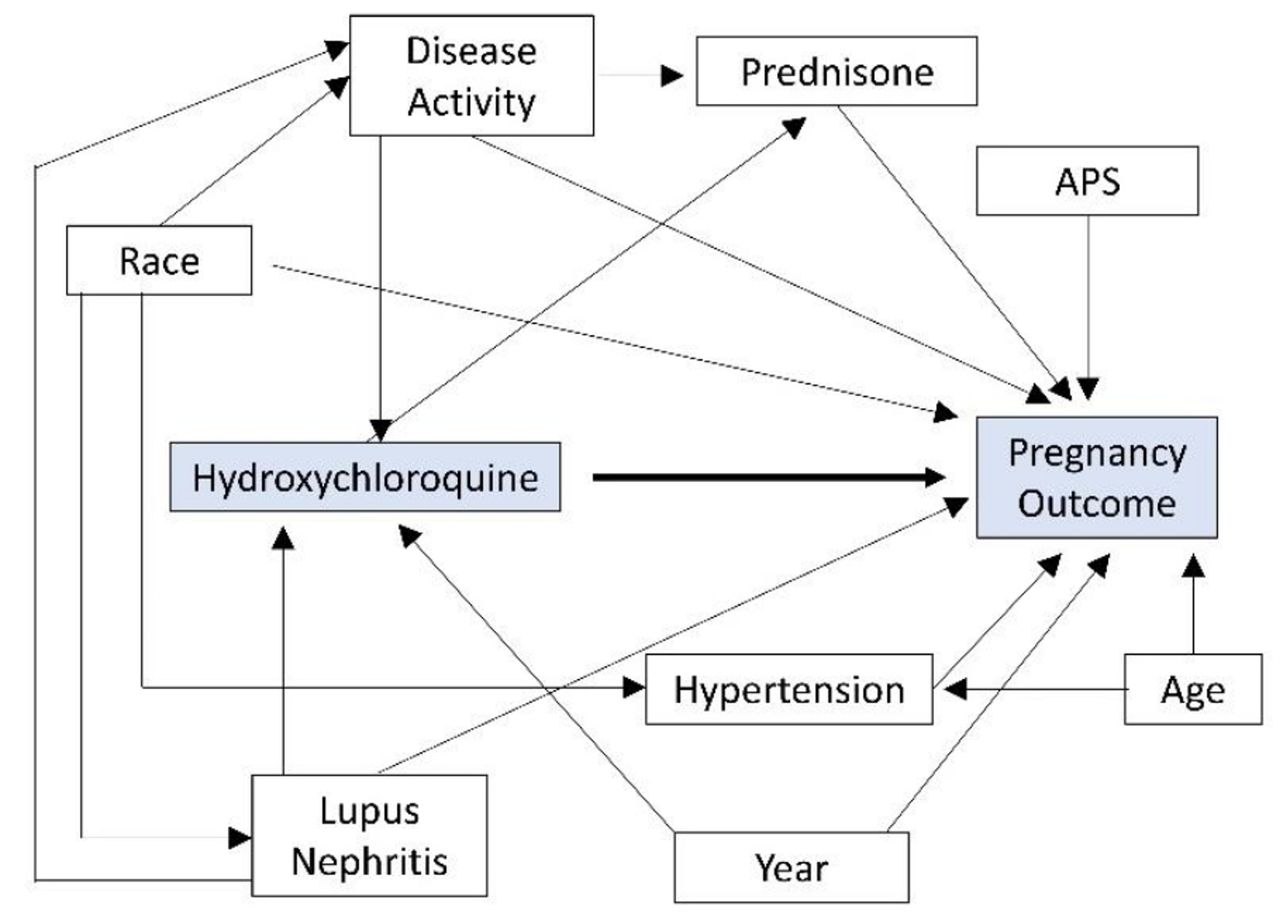
Directed acyclic graph demonstrating the influence of confounders on hydroxychloroquine (HCQ) use and pregnancy outcomes. Adjustments were made for disease activity and lupus nephritis, as both influence HCQ prescription and pregnancy outcomes. While hypertension, race and maternal age impact pregnancy outcomes, they do not strongly influence HCQ prescription, so adjustment is not required in this analysis. Year of pregnancy could impact both HCQ prescription and pregnancy outcomes based on changes in practice over time; however, the lead physicians in each study did not significantly alter HCQ prescribing habits during the study period so this was excluded from the analysis. APS, antiphospholipid syndrome.
Risk of bias assessment
The study was assessed for bias by the study team using the Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I).27
Results
Study selection
Once the inclusion and exclusion criteria were applied, we identified 40 potential cohorts which ultimately resulted in nine investigators eligible and interested in participating and seven who were able to contribute datasets (figure 1). The most common reasons for the lack of participation was study ineligibility due to either lack of consent or retrospective data collection (n=11), followed by investigators who did not respond to repeated inquiry (n=10).
Study characteristics
Seven cohorts were all collected prospectively through specialised university rheumatology clinics. A total of 962 pregnancies in 821 women were obtained from seven cohorts; 761 (79%) of pregnancies in 668 women had a first trimester visit and the frequency of first trimester visits ranged between 61% at Duke University and 100% in Israel (table 1).
Cohort characteristics
There were important variations between the women’s characteristics, medications prescribed and pregnancy outcomes between the cohorts. Race was recorded in four cohorts, the frequency of APS varied widely and a one-third of all pregnancies occurred in a woman with a history of LN.
HCQ was the most commonly prescribed medication, with the majority of women taking this drug throughout pregnancy. The Israel, Toronto and Germany cohorts had fewer than 50% of women on this medication. Prednisone was the next most common prescription followed by azathioprine.
Pregnancy loss occurred in 12%, ranging from 2% in Italy to 23% in Israel. Preterm delivery occurred in 28% of all live births and pre-eclampsia in an estimated 12%. High SLE activity was present in 26% of all pregnancies, but just 2% of Italian pregnancies and 41% of Egyptian pregnancies.
IPD integrity
Missing data, in particular missing pregnancy outcomes, medications and disease activity, significantly decreased the number of pregnancies in the cohorts that were available for study.
Bias assessment
Using the ROBINS-I method, the overall study has a serious risk of bias, driven by confounding by indication and the unknown, but likely significant, frequency for non-adherence with HCQ.
Results of syntheses
HCQ decreased the odds of high disease activity during pregnancy among women taking HCQ (OR: 0.53; 95% CI: 0.31 to 0.93). HCQ did not, however, impact the pregnancy outcomes of fetal loss, preterm delivery or pre-eclampsia in the overall population of pregnancies in women with lupus (table 2; figure 3).
Summary of pooled ORs for the association of HCQ with pregnancy outcomes among women with lupus

{kind=link}
{kind=link}
{kind=link}
Forest plots for the effect of hydroxychloroquine (HCQ) use on pregnancy outcomes in women with SLE.
Subgroup analysis: When the analysis was stratified by disease activity in the first trimester, those with low disease activity early in pregnancy who took HCQ had a decreased odds of preterm delivery (OR: 0.55; 95% CI: 0.30 to 0.99). On the other hand, HCQ use did not appear to impact the odds of preterm delivery among women with more active SLE in the first trimester. Whether a woman had high lupus activity in her first trimester or not, HCQ did not impact the odds of fetal loss or pre-eclampsia.
Results were similar when the analysis was restricted to women with prior or current LN. High disease activity was reduced among women with a history of LN taking HCQ, but HCQ was not significantly related with fetal loss, preterm delivery or pre-eclampsia in women with or without a nephritis.
Among women with and without APS, HCQ remained unrelated to fetal loss, preterm delivery or pre-eclampsia, but there was a decreased odds of high disease activity during pregnancy among women without APS.
A reanalysis using a different random selection of pregnancies (one per woman) produced the same results, with no significant association between HCQ use and fetal loss, preterm delivery or pre-eclampsia but a decreased odds of high disease activity in women taking HCQ. In sensitivity analyses assuming (1) all women with missing pre-eclampsia data had pre-eclampsia and (2) all women with missing pre-eclampsia data did not have pre-eclampsia, we did not observe an association between HCQ and pre-eclampsia overall or in any subgroup analyses.
Discussion
By combining datasets from seven prospective lupus pregnancy cohorts in an IPD meta-analysis, we found that taking HCQ throughout pregnancy decreased the odds of high SLE activity in pregnancy and had no impact on fetal loss, preterm delivery or pre-eclampsia. Among women with low SLE activity early in pregnancy, taking HCQ was associated with a lower odds of preterm delivery; this benefit was not found in women with highly active SLE. Three prior systematic reviews and/or meta-analyses including a range of studies, though none using a patient-by-patient analysis as we have employed, each reached a similar conclusion: HCQ did not significantly impact pregnancy outcomes.28–30 Specifically, these studies noted that prematurity, intrauterine growth restriction, congenital malformations, low birth weight and stillbirth were not associated with HCQ. Only one analysis identified a higher risk of early pregnancy loss in women with HCQ, but this was not confirmed in another analysis nor in this analysis. While we were not able to include data from the PROMISSE study, the results of this multicentre prospective study were similar, with no difference in the frequency of adverse pregnancy outcomes in women with and without HCQ use.31
Several recent studies have suggested pregnancy benefits from HCQ beyond SLE. Three recent studies suggested that HCQ may play a role in improving pregnancy outcomes for women with APS; we did not see a benefit from HCQ in 97 women with both SLE and APS.32–37 A clinical trial is currently underway testing the efficacy of HCQ in women with refractory APS.38 One retrospective study and a meta-analysis demonstrated a decrease in pre-eclampsia among women with lupus taking HCQ in pregnancy; we did not find a similar benefit studying 65 SLE pregnancies with pre-eclampsia, the largest dataset available.9 39 Finally, HCQ has been demonstrated in several retrospective studies and one prospective study to significantly decrease the incidence of congenital heart block (CHB) due to maternal Ro/SSA antibodies; this study did not include a sufficient number of CHB cases to study this association.40–44
This meta-analysis does not address congenital defects or long-term infant outcomes because the cohorts were not designed for systematic ascertainment of congenital defects nor the infant outcomes beyond the several weeks after delivery. Several recent studies, however, have assessed the risk of congenital defects with HCQ or chloroquine exposure in large administrative databases with varying results. While a large study of two US national databases found a significant increase in birth defects, no increase was found in similar studies from Denmark, Quebec, two US state-based datasets or an Israeli teratology study.12–15 45 Ocular toxicity from in utero exposure has not been identified in 12 cohorts and randomised trials.46
An important strength of this paper is that, by having access to the individual patient-level data, we were able to run similar analyses on each dataset so that our analysis was not restricted to previously published study results. A key strength of this project is the prospective collection of pregnancies, with disease activity and medications recorded prior to delivery. Additionally, all pregnancies were enrolled in the first trimester and managed by a rheumatologist with a particular interest in pregnancy management, suggesting that, within each centre, patients received similar, state-of-the art care with or without HCQ therapy. By including multiple centres, this study incorporates pregnancies from across the globe and enhances the generalisability of the study to multiple races and ethnicities of patient.
Despite reporting on the largest, detailed, prospectively collected set of lupus pregnancies, this study contains multiple potential biases that confound the results and conclusions. As pregnancies occurred over a 20-year period and in seven different centres, all pregnancies did not receive uniform obstetric or rheumatological care. While the majority of women were prescribed 400 mg of HCQ each day, the exact dose throughout pregnancy is not known. As HCQ is often weight based, some women may have been underdosed, particularly in light of weight gain during pregnancy.47 Bias by indication may have obscured clinical benefits of HCQ. All care was ‘standard of care’ and determined at the discretion of the treating physicians and pregnant women; women were not randomised to HCQ. Women with mild lupus and the lowest risk for pregnancy complications may have been less likely to be prescribed HCQ, thus improving the pregnancy outcomes for the non-HCQ group. In a subanalysis women with either current or prior LN, who likely all have a uniform indication for HCQ, HCQ was not associated with significantly different pregnancy outcomes. Missing data points were not unusual as each of these studies was collected as an adjunct to clinical care and led to the need to exclude some pregnancies from the analysis. We found that missing data were not random, with more women missing pre-eclampsia outcomes taking HCQ than those with documented outcomes. In sensitivity analyses, these missing data did not change our conclusion that HCQ did not impact the rate of pre-eclampsia. Few cohorts contained detailed information about parity, preventing an analysis of first pregnancies. First pregnancies can have higher rates of complications compared with later pregnancies due to the biological increased risk for pre-eclampsia in first pregnancies, but also differences in pregnancy planning, SLE and pregnancy care, and the timing of presentation to expert care. Each cohort was designed independently and collected different data, preventing adjustment for a broad range of confounders.
Our study could not account for adherence and it is likely that some women who did not actually take the drug were included in the HCQ group. Outside of pregnancy, 18%–44% of patients with SLE who report taking HCQ are not taking it based on blood HCQ levels.48–50 In 25 women with SLE within the DAP Registry (Duke University), 24% of women who reported taking HCQ had levels demonstrating non-adherence; preterm delivery occurred in 83% of non-adherent mothers compared with 21% of adherent mothers (p<0.01).51 Based on these prior studies, we estimate that about a quarter of women in the HCQ group of each cohort may be non-adherent and are thus missclassified in the HCQ group. Assuming that these non-adherent pregnancies have the same rate of poor pregnancy outcomes as pregnancies in women not taking HCQ, the actual pregnancy outcomes for women taking HCQ may be better than currently reported. Given the size of this variability, this missclassification could obscure any clinical benefit from HCQ. Overcoming this bias at this point is not possible, but future prospective studies should include measurements of HCQ levels to better classify medication use.
In summary, this is the largest, prospective study of SLE pregnancy, including seven cohorts with over 900 pregnancies collected worldwide over the last several decades. Using an independent patient-level meta-analysis, we found that HCQ use throughout pregnancy was associated with decreased SLE activity, but was not associated with pregnancy loss, preterm delivery and pre-eclampsia. Among women with low SLE activity in the first trimester, however, HCQ was associated with lower odds of preterm delivery. Given the near ubiquity of HCQ therapy in young women with SLE and the demonstrated benefit in lupus activity from continued HCQ in pregnancy, the finding that continuing HCQ in pregnancy does not negatively impact pregnancies is reassuring. Potential biases of indication, missing data and non-adherence are serious limitations to this and all currently available data on HCQ use in lupus pregnancy. These limitations can only be overcome through a large, randomised, double-blind trial of HCQ in lupus pregnancy that includes frequent measurements of HCQ levels; given the established role of HCQ in lupus pregnancy management, however, such a trial may not be feasible. Taken together, this study supports the current recommendations from the American College of Rheumatology, EULAR, British Rheumatology Association to continue HCQ during lupus pregnancy.16 18 19 52
Data availability statement
Data are available on reasonable request from the principal investigators of each study.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Duke University IRB (No: Pro00066961). Participants gave informed consent to participate in the study before taking part.
References
Footnotes
Contributors MC: Conceptualisation; methodology; guarantor; collection and curation of clinical data; writing—original draft; funding acquisition. AE: Conceptualisation; methodology; formal analysis; data curation; writing—review and editing; visualisation. SB: Investigation; writing—review and editing. GS-S: conceptualisation; methodology; supervision. AK: Methodology; validation; data curation. RF, DDG, MU, YM, CN, AT, AM, MAP: Methodology; collection and curation of clinical data; writing—review and editing. CB: Writing—Review and editing; visualization. MvN: Methodology; data curation; investigation.
Funding National Center for Advancing Translational Sciences (1KL2TR002554), National Institute of Arthritis and Musculoskeletal and Skin Diseases (AR069572), Arthritis Foundation and Arthritis Investigator Award, AHRQ (1K18HS023443-01A1).
Competing interests MC: Funding: AHRQ, Arthritis Foundation; Grants: GSK; Consulting and Advisory Board: UCB. AE: Grant funding: NIH NCATS Award 1KL2TR002554. SB: Grants: NIH, US FDA, PCORI, RRF, CARRA; Consulting: UCB; Travel: FDA; Leadership: CARRA Assistant Scientific Director. DDG: Grants and/or consulting fees from AstraZeneca; Leadership: Member of the Systemic Lupus International Collaborating Clinics group; served on the Medical advisory board of the Lupus foundation of America. MAP: Grant NIH RO-1 AR069572.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.