Article Text

Abstract
Background and Aims Juvenile systemic lupus erythematosus (SLE) and Kawasaki disease can have several overlapping clinical and laboratory manifestations. But the co-occurrence of both disorders is extremely uncommon.
Methods To report the case of a young boy who had features of both SLE and KD
Results A 5 year old boy presented with fever for 2 months associated with photosensitive malar rash, oral ulcers and myalgias.On examination, he was irritable, had malar rash, a generalised erythematosus macular rash, oral ulcers, red and vertically cracked lips, redness of bulbar conjunctiva, cervical lymphadenopathy and hepatomegaly. Laboratory investigations are summarised in Table 1. All infectious disease workup was normal. He had hypocomplementemia, positive ANA, anti dsDNA and anti-nucleosome antibody. He was diagnosed as SLE and initiated on oral prednisolone. Fever subsided, transaminitis and leucopenia showed gradual recovery. One week later developed periungual skin peeling and he remained irritable. Laboratory investigations showed anaemia, thrombocytosis, persistently elevated ESR and high CRP (Table 1) A diagnosis of incomplete KD was proffered. He was given intravenous immunoglobulin (IVIG) (2 gm/kg), which led to prompt improvement in his irritability. He was initiated on aspirin (3 mg/kg/day) and continued on oral prednisolone. Aspirin was discontinued 6 weeks later after confirmation of normal coronary findings on echocardiography. Beau’s lines were noticed in the finger nails at this time. At 3 months follow-up, he continues to remain well. Serum transaminases, platelet counts, ESR and CRP have normalised. (Table 1)
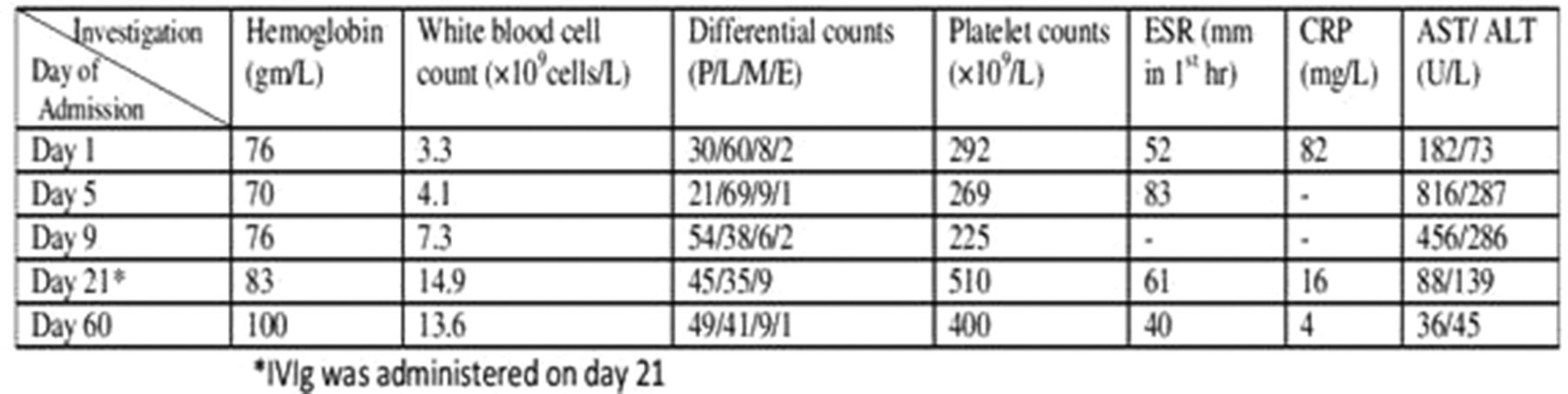
Laboratory investigations
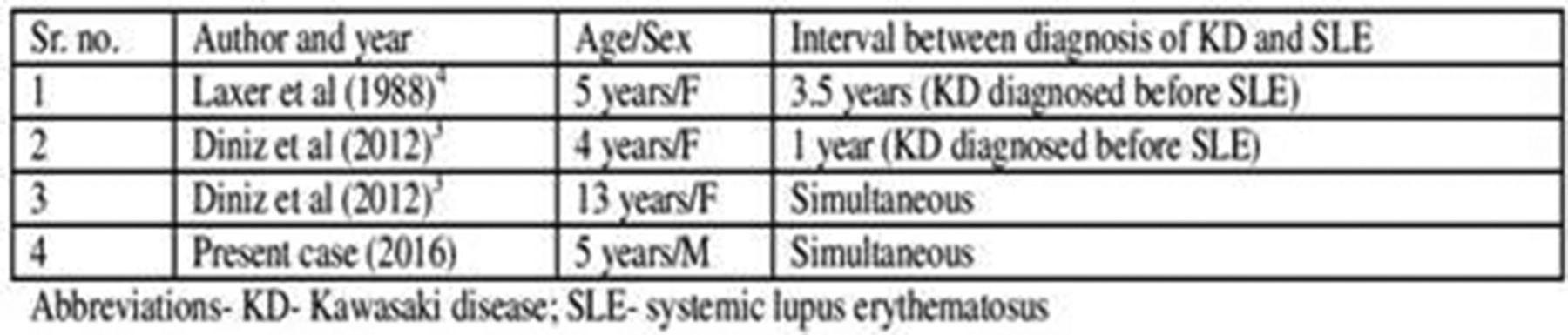
Conclusions Overlap of KD and SLE is extremely uncommon. (Table 2)

{kind=link}
{kind=link}