Article Text

Abstract
Background and aims Several different versions of classification criteria, including the American College of Rheumatology (ACR)-1997, Systemic Lupus International Collaborating Clinics (SLICC)-2012 and European Alliance of Associations for Rheumatology (EULAR)/ACR-2019 classification criteria, have been launched in the past decades. The current study aimed to investigate the performance of these three classification criteria for diagnosing patients with SLE in a Chinese cohort.
Methods 352 patients with SLE and 385 controls with other diseases who had the detection results of ANA were enrolled into the study. Various clinical parameters were estimated, such as demographics variables, clinical characteristics and other variables related to three criteria.
Results The current study demonstrated great diagnostic ability of the three criteria; and the receiver operating characteristic curve and the area under curve (AUC) were used to evaluate the diagnostic ability of three criteria: ACR-1997 (AUC=0.972), SLICC-2012 (AUC=0.986) and EULAR/ACR-2019 (AUC=0.983). Despite lower specificity of the SLICC-2012 and EULAR/ACR-2019 classification criteria, their sensitivity is significantly improved than ACR-1997. Of note, we also compared the median time interval between the appearance of the earliest item and fulfilment of the three sets of criteria, suggesting the SLICC-2012 and EULAR/ACR-2019 could achieve earlier diagnosis. Adjusting the thresholds of the EULAR/ACR-2019 criteria from 10 to 12, the specificity and accuracy significantly increased.
Conclusion The SLICC-2012 and EULAR/ACR-2019 performed well in Chinese patients with SLE and showed better early diagnosis ability. In addition, by adjusting the classification threshold, the accuracy of the EULAR/ACR-2019 classification criteria was improved.
- lupus erythematosus, systemic
- lupus nephritis
- autoimmune diseases
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
SLE classification criteria are currently used for assisting in diagnosing relatively homogeneous patients as SLE, including the American College of Rheumatology (ACR)-1997, Systemic Lupus International Collaborating Clinics (SLICC)-2012 and European Alliance of Associations for Rheumatology (EULAR)/ACR-2019 classification criteria.
WHAT THIS STUDY ADDS
The SLICC-2012 and EULAR/ACR-2019 performed well in Chinese patients with SLE and showed better early diagnosis ability. Adjusting the thresholds of the EULAR/ACR-2019 criteria from 10 to 12, the specificity and accuracy significantly increased.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The EULAR/ACR-2019 has a good application prospect for SLE in the Chinese cohort. Early confirmation of SLE may allow for provision of early intervention, effectively prevent the progression and reduce damage from complications.
Introduction
SLE is characterised as a multisystem autoimmune disease with high clinical heterogeneity as well as unpredictable course and flares.1 2 Despite the improved prognosis of patients with SLE, failure in promptly diagnosing contributes to a proportion of patients progressing in severity and/or to treatment delay, even no treatment.2 Moreover, the mortality of SLE presents a ‘bimodal pattern’; the early death is due to disease activity and secondary infection, and the late death is mainly attributed to cardiovascular disease and organ failure.3 Therefore, the timely diagnosis of patients in the early stage of the disease is conducive to early treatment, so as to achieve the purpose of alleviating the disease, delaying disease progress and reducing the incidence of complications, thereby reducing the medical pressure of both patients and society. It follows that timely and accurate diagnosis is critical for patients with SLE but remains a major challenge.4
Of note, there are no well-defined diagnostic criteria currently used for assisting in diagnosing relatively homogeneous patients as SLE but rather classification criteria. To date, several different versions of classification criteria, primarily based on the sum of clinical presentations, serum immunological or inflammatory parameters, radiological features and histopathological analyses, have been launched in the past decades, represented by American College of Rheumatology (ACR)-1997 classification criteria,5 Systemic Lupus International Collaborating Clinics (SLICC)-2012 classification criteria6 and European Alliance of Associations for Rheumatology (EULAR)/ACR-2019 classification criteria7 8 (these three classification criteria are expressed in chronological order).
Of the widely accepted and applied criteria for SLE, ACR-1997 criteria was developed based on updates of the version by ACR in 1982 (ACR-1982 classification criteria).9 Given the limitations of the former, a new set of criteria was proposed by the SLICC experts in 2012.6 The main and obvious distinction between the two proposals lies in clinical and immunological items; notably, ‘renal lupus only’ cases with positive ANA or anti-double-stranded DNA antibodies should be classified as SLE according to the SLICC-2012,6 and in the contrary, they cannot meet the diagnosis according to the items of the ACR-1997 classification criteria.5 9 Subsequently, in 2019, the EULAR and ACR joined forces to formulate new SLE classification criteria. It takes ANA titre ≥1:80 as the necessary admission item, followed by seven items of clinical manifestations and three items of immunological indicators. Each item corresponds to a weighted score. A total score of at least 10 allows for a diagnosis of SLE.7 8 The EULAR/ACR-2019 classification criteria is designed to identify early SLE, so non-infectious fever is a new item given its higher incidence rate in patients with early SLE than in patients without SLE (34.5% vs 13.7%).7 8 The diagnostic performance of the EULAR/ACR-2019 classification criteria has been investigated in some studies.7 10–16 A study conducted by Petri et al showed that the diagnostic ability was 90.0%14; and in the recent case–control study, the diagnostic accuracy of EULAR/ACR-2019 classification criteria reached 91.8%.15 Johnson et al demonstrated that the diagnostic accuracy of the EULAR/ACR-2019 was 95.4%. In addition, the study showed that sensitivities of the three sets of classification criteria in Hispanic population were higher than those in white, black and Asian population; compared with white, Hispanic and Asian population, black population had the best specificity.12 As such, there are differences in diagnostic performance by using the existing classification criteria to diagnose patients with SLE in different races.
Despite wide utilisation of these three sets of classification criteria by Chinese clinicians, the data on their performance in the diagnosis of patients with SLE in China are scant to the best of our knowledge. Therefore, the performance of SLE classification criteria in Chinese population needs further investigation. Herein, the current study aimed to compare the performance of the EULAR/ACR-2019, SLICC-2012 and ACR-1997 classification criteria for diagnosing patients with SLE in a Chinese cohort. Moreover, their ability of early diagnosis was further investigated by comparing the time to classification and time to diagnosis.
Methods
Participants
This retrospective observational study included patients with and without established SLE, recruited from the Department of Rheumatology and Immunology at the Second Affiliated Hospital of Soochow University between January 2016 and December 2020. All the patients with SLE were diagnosed by consultant rheumatologists with ≥8 years of clinical practice according to patients’ clinical symptoms, signs and the results of laboratory examination and imaging examination.9 The exclusion criteria of the case group were as follows: (1) combined with other connective tissue diseases, such as rheumatoid arthritis, systemic sclerosis, Sjogren’s syndrome, Behcet’s disease, etc; (2) with infection, liver cirrhosis, pregnancy, malignant solid or blood tumour; (3) lack of follow-up data; (4) missing important clinical or laboratory data to assess the classification criteria. In addition, individuals with ANA test results but diagnosed as other diseases by the same rheumatologists were selected into the control group, including Behcet’s disease, primary Sjogren’s syndrome, undifferentiated connective tissue disease, systemic sclerosis, rheumatoid arthritis, rheumatic polymyalgia, immune thrombocytopenic purpura, inflammatory bowel disease, malignant tumour and infection. Those with incomplete clinical or laboratory data were excluded.
Data collection
Demographic, clinical symptoms, signs, laboratory tests, time-related and other data associated with the EULAR/ACR-2019, SLICC-2012 and ACR-1997 classification criteria were collected from electronic medical recording; and the total score was calculated respectively. During the project establishment and training of data collectors, this study emphasised that attention should be paid to the identification of similar diseases when collecting clinical data such as symptoms and signs. If there was a more alternative explanation, it would not be considered as a positive item of the classification standard. After the collection of research data and before the start of research analysis, another staff member was arranged to recheck the clinical data. If there was any doubt, it would be confirmed again by the two clinical experts to avoid attribution errors as far as possible. ANA titre was measured by using immunofluorescence antibody assay in our centre. Positive ANA was set at a serum dilution of ≥1:100 in the immune laboratory of the Second Affiliated Hospital of Soochow University.
Statistical analysis
All the variables in the study were described by count with proportion or median with minimum and maximum (depending on the type and distribution of variables). The differences between independent groups were assessed by Student’s t-test, Mann-Whitney U test, Χ2 test or Fisher’s exact test. According to the clinical judgement of rheumatology experts, sensitivities, specificities, accuracies, positive predictive values (PPVs), negative predictive values (NPVs), positive likelihood ratio (+LR) and negative likelihood ratio (−LR) of three classification criteria sets were calculated to evaluate and compare their diagnostic accuracy.17 By drawing the receiver operating characteristic curve of the three sets of classification criteria and calculating the area under curve (AUC), the diagnostic value of the three sets of classification criteria was compared.18 In order to improve the operation performance of the EULAR/ACR-2019 classification criteria by adjusting the classification threshold, we calculated the sensitivity, specificity and accuracy of EULAR/ACR-2019 classification criteria when the classification thresholds are 8, 9, 11, 12 and 13, respectively.
In this study, the time to diagnosis and time to classification of the three sets of classification of all patients with SLE with detailed records of clinical manifestations or abnormal occurrence time of laboratory examination were calculated. The time to diagnosis was defined as the time interval from the first occurrence of SLE-related symptoms or abnormal laboratory test results to clinical diagnosis, and the time to classification as the time interval from the first occurrence of an item to meeting the threshold specified in the classification criteria. The study compared the time to diagnosis and the time to classification of the three classification criteria, and investigated their differences in different gender and age groups. At the same time, the groups were compared according to the involved system. The Kaplan-Meier curve was drawn with meeting the ACR-1997, SLICC-2012 and EULAR/ACR-2019 classification criteria as the outcome event. P value of <0.05 is considered to be the statistically significant between groups, and the CI of the estimated value is 95%. Statistical analysis was performed using IBM SPSS V.26.0 software (International Business Machines Corporation), MedCalc V.19.7.2 software (Ostend, Belgium) and GraphPad Prism V.8.0.0 software (San Diego, California, USA).
Results
Patients’ characteristics
During the study interval, there were 352 patients with SLE (SLE group) and 385 individuals without SLE (control group) enrolled into our study. The baseline characteristics between the two groups are presented in table 1. Of the total 737 patients, the majority of patients were female, with 322 (91.5%) and 279 (72.5%) in the SLE and control group, respectively.
The baseline characteristics of patients in SLE group and control group
Patients with SLE were significantly younger than those in the control group (median age: 36.0 vs 54.0; p<0.001), and individuals aged <40 years accounted for 58.0% and 22.9%, respectively. In the SLE group, the course of disease ranged from a week to 37 years, with the most patients over 5 years (59.1%), followed by patients less than 1 year (23.9%).
Of the eight items in ACR-1997 criteria, there were significant differences in the clinical variables between the SLE versus the control groups, apart from discoid rash (p=0.511). Among the SLICC-2012 criteria, 16 of 17 items between the two groups were observed to be significantly different, except for chronic cutaneous lupus (p=0.511). Given the number of patients with discoid rash/chronic cutaneous lupus was too small (two in case group and one in control group), effective statistical analysis cannot be performed. Of the 11 variables in EULAR/ACR-2019 criteria, there were significant differences between the two groups (table 1).
Diagnostic ability of different classification criteria
Our study further investigated the classification accuracy of the ACR-1997, SLICC-2012 and EULAR/ACR-2019 classification criteria. Of the total 352 patients with SLE, 289 (82.1%), 345 (98.3%), and 343 (97.4%) reached criteria for ACR-1997, SLICC-2012, and EULAR/ACR-2019 criteria, respectively. Moreover, 287 met all three sets of classification criteria, and in contrast, 3 patients did not meet any one. The values of AUC, sensitivity, specificity, accuracy, PPV, NPV, and LR were shown in table 2 and figure 1. Based on the clinical practice, 4, 4, and 10 scores were used as the cut-off values of ACR-1997, SLICC-2012, and EULAR/ACR-2019 criteria, respectively. As shown in figure 1, the three criteria all had excellent classification ability; and the SLICC-2012 and EULAR/ACR-2019 criteria yielded the optimal performance with the AUC (95% CI) of 0.986 (0.975 to 0.993) and 0.983 (0.970 to 0.991) (p=0.459), followed by ACR-1997 (AUC=0.972 (0.957 to 0.983); vs SLICC-2012, p=0.001; vs EULAR/ACR-2019, p=0.016); and SLICC-2012 and EULAR/ACR-2019 had the excellent diagnostic accuracy with the values of 95.0% (93.1% to 96.4%) and 94.3% (92.4% to 95.9%), respectively, compared with ACR-1997 (89.6% (87.1% to 91.7%)). Of the three criteria, ACR-1997 presented the highest specificity of 96.4% (vs 92.2% for SLICC-2012 and 91.4% for EULAR/ACR-2019), but the lowest sensitivity of 82.1% (vs 98.0% for SLICC-2012 and 97.4% for EULAR/ACR-2019).
Operating characteristics of the ACR-1997, SLICC-2012 and EULAR/ACR-2019 classification criteria in the SLE and control cohorts

The diagnostic performance of the ACR-1997, SLICC-2012 and EULAR/ACR-2019 in patients with ANA-positive SLE and controls. ACR, American College of Rheumatology; EULAR, European Alliance of Associations for Rheumatology; SLICC, Systemic Lupus International Collaborating Clinics.
Gender, ages and disease duration
The sensitivity and specificity of the three SLE classification criteria following the stratification for gender and age were described in table 3. Whether in the male or female subgroup, both the SLICC-2012 and EULAR/ACR-2019 criteria yielded higher sensitivity and lower specificity than ACR-1997 (sensitivity: 100.0% vs 90.0% vs 89.1% for male; 98.1% vs 98.1% vs 82.0% for female; specificity: 96.2% vs 96.2% vs 100.0% for male; 90.7% vs 89.6% vs 95.0% for female). In the two subgroups of age with 40 years as the boundary, a lowest sensitivity and a higher specificity were observed in ACR-1997 criteria compared with SLICC-2012 and EULAR/ACR-2019 criteria. Regardless of the definition of disease duration, both SLICC-2012 and EULAR/ACR-2019 criteria presented better sensitivities (ranging from 95.7% to 100.0%), but ACR-1997 performed less well with sensitivities ranging from 78.6% to 81.8%. In patients with SLE with courses of no more than 5 years, the sensitivity of SLICC-2012 and EULAR/ACR-2019 can reach 100%; the sensitivity of these two sets of classification criteria, however, decreased in the subgroup with longer disease duration (table 3).
Sensitivity and specificity of SLE classification criteria following the stratification for sex, age and disease duration
The SLICC-2012 and EULAR/ACR-2019 allowing for earlier diagnosis than the ACR-1997
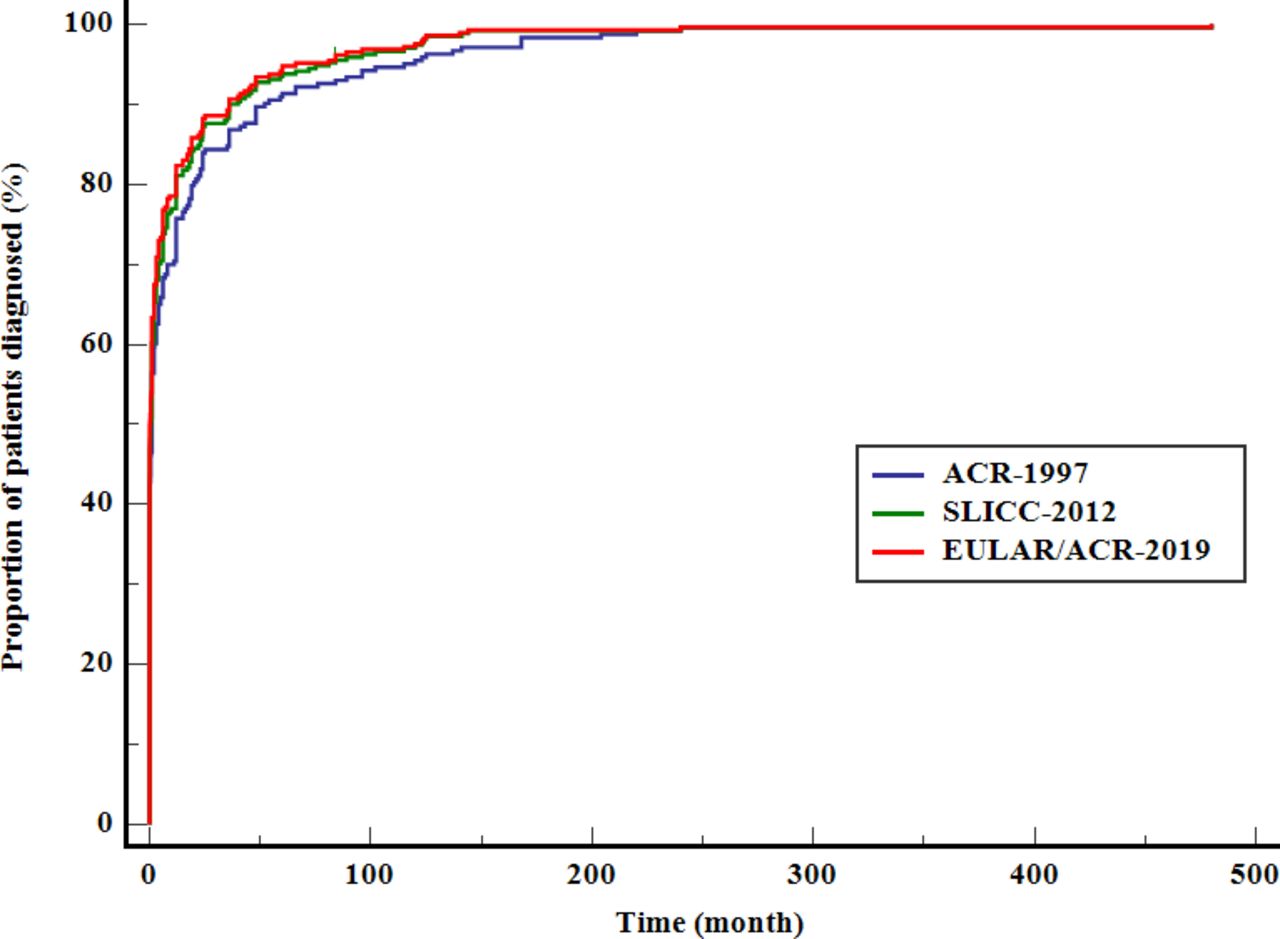
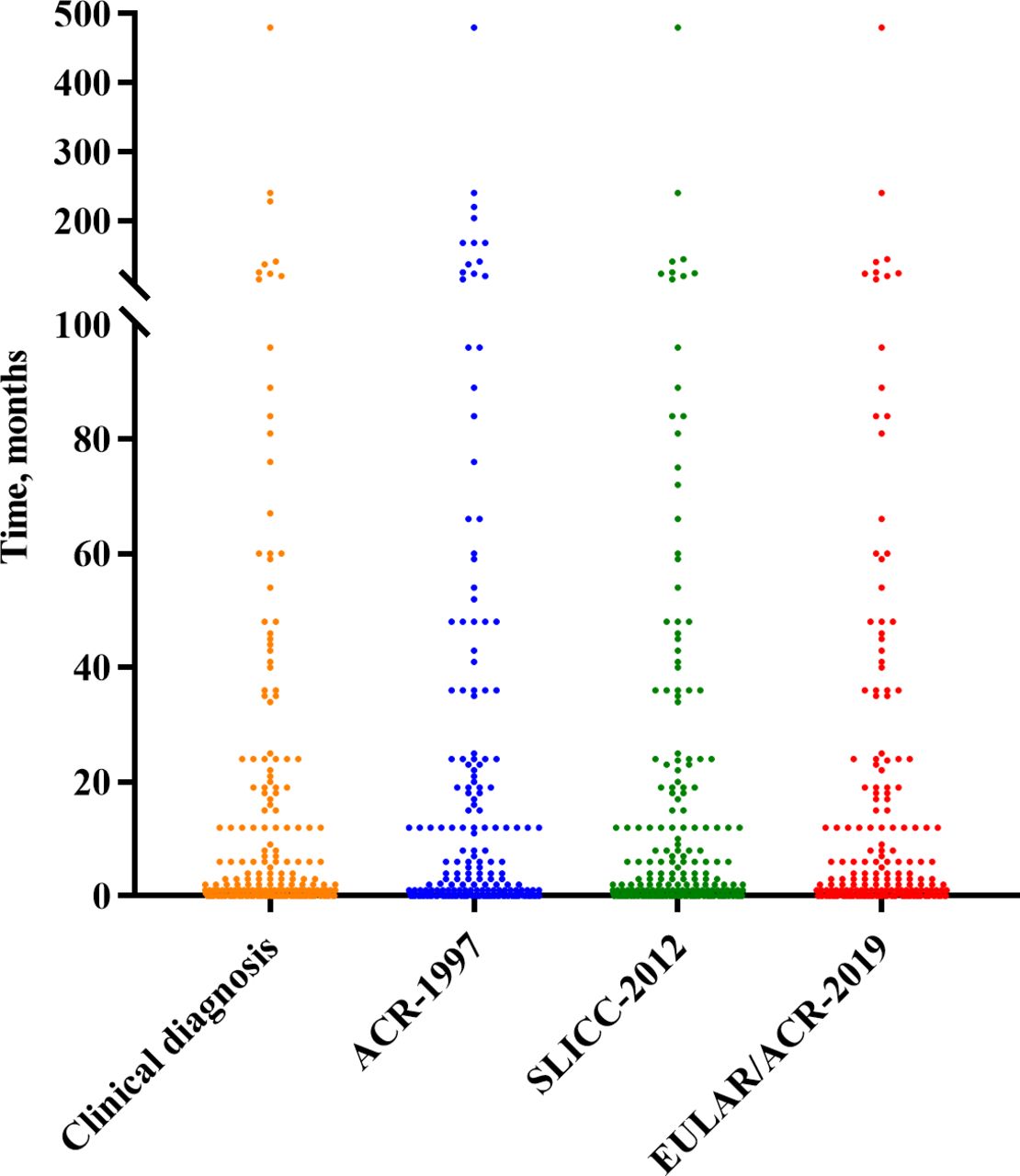
As defined above, the time to classification was defined as the time interval from the first occurrence of an item to meeting the threshold specified in the classification criteria. In the subgroup analysis of 352 patients with SLE, the shorter median time to classification was observed in the EULAR/ACR-2019 (0.13 (0.0–480.0) months) and SLICC-2012 (0.5 (0.0–480.0) months) in comparison with the ACR-1997 (1.0 (0.0–480.0) months) (figure 2). The difference between them was statistically significant (p=0.001). During the whole follow-up period, the diagnostic rates of ACR-1997, SLICC-2012 and EULAR/ACR-2019 were 82.1%, 98.0% and 97.4%, respectively. Taking meeting the three sets of classification criteria as the outcome event, the Kaplan-Meier curves were drawn in figure 3. No statistically significant difference among the three groups was observed (p=0.076).
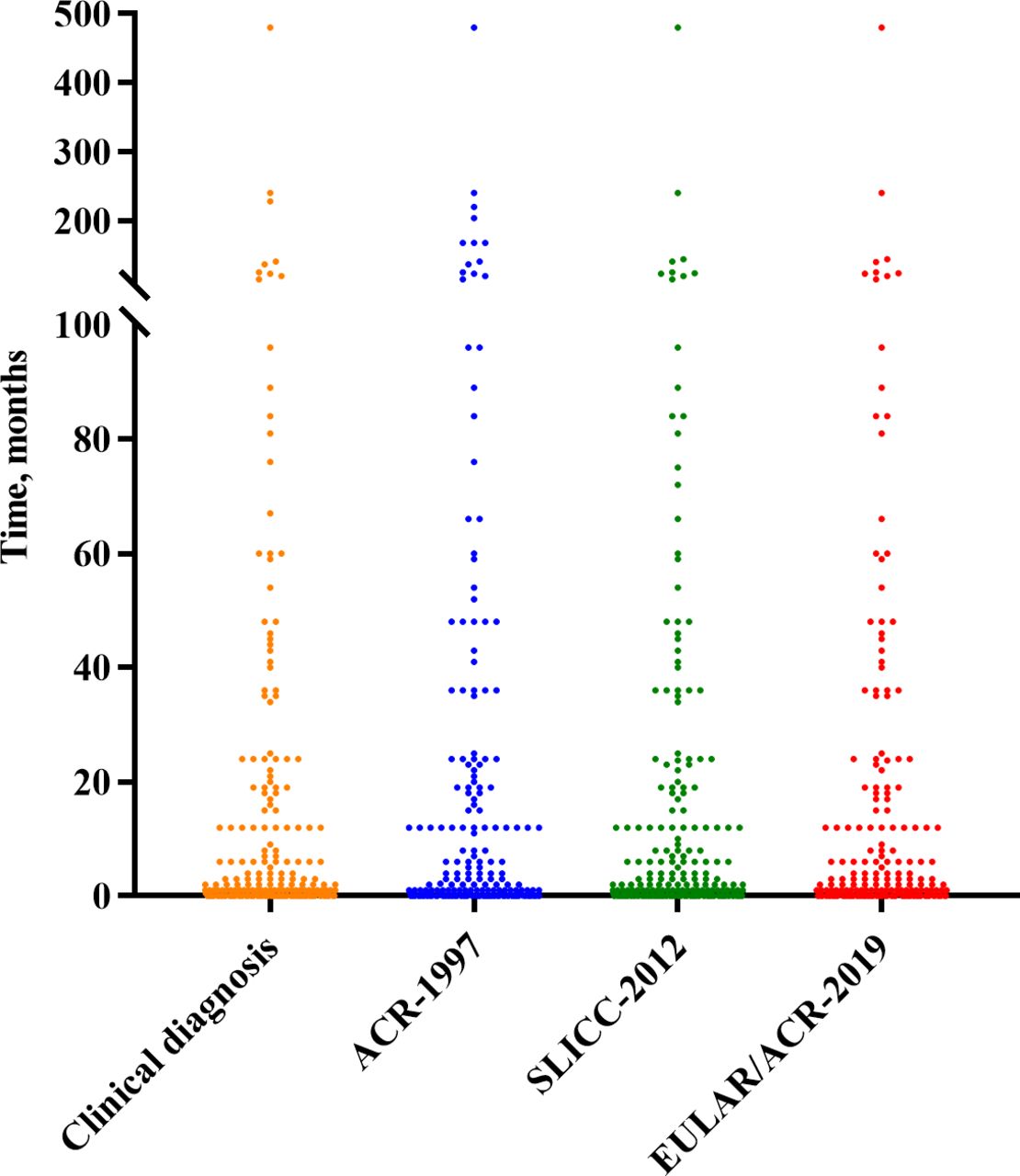
Time to classification of the ACR-1997, SLICC-2012 and EULAR/ACR-2019 classification criteria against clinical diagnosis within classified patients with SLE. In the subgroup analysis of 352 patients with SLE, the shorter median time to classification was observed in the EULAR/ACR-2019 (0.13 (0.0–480.0) months) and SLICC-2012 (0.5 (0.0–480.0) months) in comparison with the ACR-1997 (1.0 (0.0–480.0) months). ACR, American College of Rheumatology; EULAR, European Alliance of Associations for Rheumatology; SLICC, Systemic Lupus International Collaborating Clinics.
{kind=link}
{kind=link}
{kind=link}
The Kaplan-Meier curves with meeting the ACR-1997, SLICC-2012 and EULAR/ACR-2019 classification criteria as the outcome event. ACR, American College of Rheumatology; EULAR, European Alliance of Associations for Rheumatology; SLICC, Systemic Lupus International Collaborating Clinics.
In order to further clarify the early diagnosis ability of the three classification criteria, we compared the classification time of different classification criteria with the clinical diagnosis time (table 4). The time to classification of 204 cases for ACR-1997, 259 cases for SLICC-2012 and 261 cases for EULAR/ACR-2019 was the same as their clinical time to diagnosis. In contrast, 8, 17 and 19 cases were earlier than clinical diagnosis, respectively; and 33, 17 and 9 cases were later than clinical diagnosis. Therefore, SLICC-2012 and EULAR/ACR-2019 showed better early diagnosis ability.
Timing of fulfilment of the classification criteria compared with clinical diagnosis of SLE
Subsequently, we performed subgroup analysis according to the involvement system. The results showed that both SLICC-2012 with sensitivities ranging from 78.6% to 81.8% and EULAR/ACR-2019 showed optimal early diagnosis performance, whether it was skin mucosal lesions, serositis and arthritis, or the involvement of more important organs such as blood system and kidney (table 4).
The modified algorithms
Based on the different cut-off values for EULAR/ACR-2019 classification criteria (≥8, ≥9, ≥10, ≥11, ≥12, ≥13, ≥14 and ≥15), our study presented the values of sensitivity, specificity, accuracy, PPV, NPV and LR in table 5. After adjusting the thresholds of the EULAR/ACR-2019 criteria from 10 to 12, the specificity significantly increased (from 91.4% to 94.8%), the sensitivity slightly decreased (from 97.4% to 95.2%) and accuracy increased (from 94.3% to 95.0%). Furthermore, the EULAR/ACR-2019 with a threshold of 12 had better sensitivity than the ACR-1997 (95.2% vs 82.1%), better specificity than the SLICC-2012 (94.8% vs 92.2%) and similar accuracy with the SLICC-2012 (95.0% vs 95.0%), but better accuracy than the ACR-1997 (95.0% vs 89.6%).
Classification performance of the different cut-off points for EULAR/ACR criteria (≥8, ≥9, ≥10, ≥11, ≥12, ≥13, ≥14 and ≥15) in the SLE and control cohorts
Discussion
This retrospective study investigated the diagnostic efficacy of three classification criteria, that is, ACR-1997, SLICC-2012 and EULAR/ACR-2019, for SLE in a Chinese single-centre cohort. The findings in the current study demonstrated great classification abilities of the three criteria; and the SLICC-2012 and EULAR/ACR-2019 had the highest accuracy, followed by ACR-1997. Of note, the SLICC-2012 and EULAR/ACR-2019 could achieve earlier diagnosis, especially the latter one. In addition, by adjusting the classification threshold of EULAR/ACR-2019 from 10 to 12, the specificity and accuracy were improved.
In our study, there were statistically significant differences in gender composition and age distribution between the groups. The reasons for it were manifold and varied, but the one that dominated was gender and age difference of high-risk population in different diseases. Namely, the incidence of SLE in the case group was women of childbearing age.1 19–23 And in contrast, the proportion of patients with rheumatoid arthritis in the control group was large, and the incidence of rheumatoid arthritis was in middle-aged and elderly women24–28; furthermore, the control group included ankylosing spondylitis which was commonly seen in young men.29–31 In order to compare the performance of classification criteria in different gender, age and course of disease, and to eliminate the impact of differences between the case and control group, the groups were further stratified according to gender and age, and then the sensitivity and specificity of classification criteria were compared. We found the changes on sensitivity and specificity of the three sets of classification criteria in different subgroups had the same upward or downward trend. Therefore, the impact on the differences of gender composition and age distribution caused by the selection of the control group was considered little in the overall analysis.
Our study demonstrated that the clinical item of discoid erythema in ACR-1997 and chronic cutaneous lupus in SLICC-2012 was not significantly different between the case group and the control group. The finding rests chiefly on the fact that the number of patients with discoid erythema in the case group and the control group was too small to obtain statistically significant results. In the follow-up study, comparison of this item can be achieved by expanding the sample size.
Previous studies noted that the EULAR/ACR-2019 criteria had great operating characteristics (sensitivity and specificity) in patients diagnosed as SLE.12 15 32 Johnson et al reported that the sensitivity and sensitivity of EULAR/ACR-2019 were 96% and 90%.12 A Malaysian study published recently reported that the sensitivity of EULAR/ACR-2019 classification standard was 91% and the specificity was 94%.15 In the present study, EULAR/ACR-2019 classification also presented the great diagnostic performance for SLE, with sensitivity, specificity, and accuracy of 97.4%, 91.4%, and 94.3%, respectively.
According to the results of our study, the AUCs (95% CI) of ACR-1997, SLICC-2012 and EULAR/ACR-2019 were 0.972 (0.962 to 0.982), 0.986 (0.979 to 0.993) and 0.983 (0.973 to 0.992), respectively. This proved that the diagnostic results of the three sets of classification criteria were highly similar to the results of clinical diagnosis (the gold standard adopted in our study). In the case group of this study, rheumatologists often referred to ACR-1997 in the process of clinical diagnosis. Therefore, the high AUC score of SLICC-2012 and EULAR/ACR-2019 had little to do with the reference use in the diagnosis process.
The qualitative results of ANA in our study came from immunology laboratory of the Second Affiliated Hospital of Suzhou University, where indirect Hep-2 immunofluorescence was used to calibrate ANA titre ≥1:100 as positive results, which was consistent with the corresponding item requirements of ACR-19975 and SLICC-2012,6 but the entry criterion of EULAR/ACR-2019 is ‘ANA at a titre of ≥1:80’.7 Theoretically, the definition of positive ANA following EULAR/ACR-2019 (ANA ≥1:80) may make the sensitivity of EULAR/ACR-2019 higher than the actual value in our study (ANA ≥1:100).
Notably, given that consensus has not yet been reached on standardised definition of ‘early’ SLE, the patients with SLE in the case group were stratified according to the course of disease (≤1 year, >1 year and ≤3 years, >3 years and ≤5 years, >5 years).Our study found that among the patients with a course of disease of no more than 5 years, the sensitivities of SLICC-2012 and EULAR/ACR-2019 were better, reaching 100%. But in the subgroup with longer course of disease, the sensitivities of the two sets of classification criteria decreased, and still higher than 95%. The sensitivities of SLICC-2012 and EULAR/ACR-2019 in the diagnosis of patients with early SLE were higher than that of late SLE. It may be that some patients with late SLE cannot accurately recall the specific situation in the early stage of onset at the last follow-up, resulting in the loss of some data and the inconsistency of classification criteria. These important data could lay the foundation for the performance of clinical trials and observational studies on SLE.
Given that the disease status of SLE may have lasted for a period of time before classification, it is very important to accurately identify patients in the early stage of onset, which is beneficial to early intervention.33–38 As such, the present study also compared the classification time of the three sets of classification criteria and the time of clinical diagnosis. The results showed that EULAR/ACR-2019 and SLICC-2012 could achieve earlier diagnosis than ACR-1997; especially EULAR/ACR-2019 was the best one (median time to classification: 0.13 vs 0.50 vs 1.00 months, respectively, p=0.001).
Previous studies also pointed out that SLICC-2012 and EULAR/ACR-2019 performed well in identifying early SLE.7 15 39 Adamichou et al recruited patients with SLE with a course of <3 years to compare the early diagnostic ability of the classification criteria. In the early stage of the disease, compared with the ACR-1997, the sensitivity of SLICC-2012 and EULAR/ACR-2019 was significantly increased (79.9% vs 91.4% vs 87.3%); and the median classification times were 12.1, 9.1 and 9.1 months, respectively.10 Selvananda and Kan included patients with SLE with a course of no more than 1 year when investigating the early manifestations of the disease. The sensitivity of ACR-1997, SLICC-2012 and EULAR/ACR-2019 was 86%, 98%, and 94%, respectively; and the sensitivity of SLICC-2012 was significantly higher than that of ACR-1997.15
In a multicentre study evaluating the causes of death in 222 patients with SLE, 31% of the deaths were attributed to active organ involvement and 33% to infection, of which the involvement of the kidney and central nervous system was the most common major cause of death.40–43 Previous research data showed that even before the classification criteria were fully met, a certain proportion of patients with SLE may have organ-dominant or organ-localised diseases, especially the nervous system, kidney and haematological.44 45 In view of this, in order to better diagnose renal-dominant SLE, SLICC-2012 first introduced renal involvement as a sufficient condition for independent diagnosis,6 and EULAR/ACR-2019 increased the weight of item with renal involvement.7 Our study showed that in all subgroups, the number of patients whose classification time of SLICC-2012 or EULAR/ACR-2019 was earlier than that of clinical diagnosis was greater than that of ACR-1997. Whether it is skin mucosal lesions, serositis, arthritis, or the involvement of important organs such as haematological and kidney, SLICC-2012 and EULAR/ACR-2019 showed better early diagnosis ability.
In addition, this study improved the accuracy of EULAR/ACR-2019 by adjusting the classification threshold. When the classification threshold was set to 12, the accuracy of the classification criteria was the highest (95.0%), which was the same as that of SLICC-2012 (95.0%). The reason why the EULAR/ACR-2019 classification threshold at the highest accuracy of this classification in this study was inconsistent with the formulated classification threshold may be ethnic differences. The majority of patients in the case group and control group analysed in the formulation of EULAR/ACR-2019 classification criteria were white, with low proportion of Asian population.7 12 Previous studies involving multiethnic differences have shown that the characteristics of SLE in Asian people were different from those in other ethnic groups indeed. A meta-analysis published in 2021 reported that Asian patients with SLE were more likely to develop Malar rash, leucopenia and thrombocytopenia than non-Asian patients. There was no difference in renal and nervous system performance between Asians and non-Asians. Photosensitivity and discoid rash were less observed in Asian patients with SLE. Compared with Indian patients with SLE, Chinese patients with SLE had a lower incidence of oral ulcer.46 What is more, DeQuattro et al pointed that the disease severity index of SLE in Asian patients was significantly higher than that in white patients, but similar to that in black and Hispanic patients.47 By adjusting the classification threshold of the criteria, it may also improve the diagnosis accuracy of patients with SLE in China. We also look forward to the further verification and comparison of the classification criteria from other centres in Asia.
There are some limitations in the present study. This is a single-centre retrospective study with its inherent defect, including selection bias. A large multicentre prospective study is required for further study. Remarkably, studies pertinent to Chinese patients are still scarce to the best of our knowledge. As such, the current study compensated for a lack of data on the clinical utility of three classification criteria, that is, ACR-1997, SLICC-2012 and EULAR/ACR-2019, for SLE in the Chinese cohort.
In conclusion, both the SLICC-2012 and EULAR/ACR-2019 had optimal diagnostic efficacy in identifying Chinese patients with SLE, whether in the overall patients or the subgroup stratified by age, gender and course of disease. Furthermore, SLICC-2012 and EULAR/ACR-2019 showed better early diagnosis ability, especially the latter one. By adjusting the classification threshold of EULAR/ACR-2019 from 10 to 12, the diagnostic accuracy and specificity can be improved.
Conclusion
The SLICC-2012 and EULAR/ACR-2019 performed well in Chinese patients with SLE and showed better early diagnosis ability. Adjusting the thresholds of the EULAR/ACR-2019 classification criteria from 10 to 12, the specificity and accuracy significantly increased.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study is based on the principles of the Helsinki Declaration. Written informed consent was obtained from each patient. Before the start of the study, the ethics committee of the Second Affiliated Hospital of Soochow University approved the study protocol. The ethical review number is JD-HG-2021-19.
Acknowledgments
We thank all the clinicians at the Department of Rheumatology and Immunology at the Second Affiliated Hospital of Soochow University for their efforts.
References
Footnotes
WL and YZ contributed equally.
Contributors The comparison of three classification criteria sets was made by WL and YZ with 352 patients with SLE and 385 control individuals who were diagnosed as other autoimmune diseases. Both authors were involved in drafting and revising the article and approved the final version to be published. All authors were involved in analysing and interpreting the data, drafting the article and revising it critically for important intellectual content, and all read and approved the final version to be published. LX is the guarantor.
Funding This work was supported by the Suzhou Science and Technology Project (SKJY2021098), the National Nature Science Foundation of China (81800622), Suzhou Health and Key Talent Project (GSWS2019011), and Jiangsu Social Development Project (BE2019663).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.